Seckl Michael J, Ottensmeier Christian H, Cullen Michael, Schmid Peter, Ngai Yenting, Muthukumar Dakshinamoorthy, Thompson Joyce, Harden Susan, Middleton Gary, Fife Kate M, Crosse Barbara, Taylor Paul, Nash Stephen, Hackshaw Allan
Michael J. Seckl, Imperial College London; Yenting Ngai, Stephen Nash, and Allan Hackshaw, Cancer Research UK and University College London Cancer Trials Centre; Christian H. Ottensmeier, University of Southampton and Southampton University Hospitals, Southampton; Michael Cullen, Queen Elizabeth Hospital Birmingham; Joyce Thompson, Heart of England Birmingham; Gary Middleton, University of Birmingham, Birmingham; Peter Schmid, Brighton and Sussex Medical School, Brighton; Dakshinamoorthy Muthukumar, Colchester Hospital, Colchester; Susan Harden, Cambridge University Hospital, Cambridge; Kate M. Fife, Peterborough City Hospital, Peterborough; Barbara Crosse, Calderdale and Huddersfield NHS Foundation Trust, Huddersfield; and Paul Taylor, University Hospital South Manchester, Manchester, United Kingdom.
J Clin Oncol. 2017 May 10;35(14):1506-1514. doi: 10.1200/JCO.2016.69.7391. Epub 2017 Feb 27.
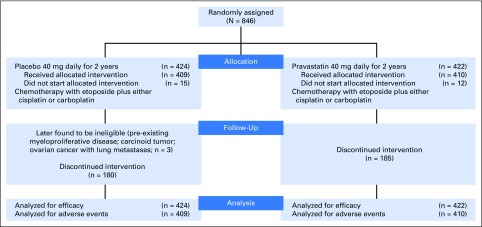
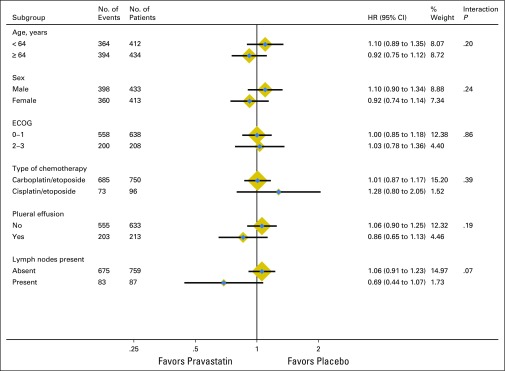
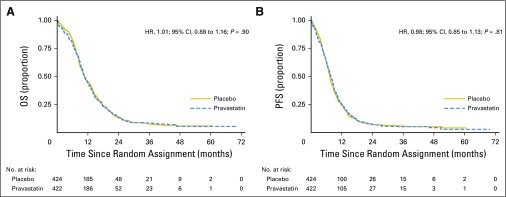
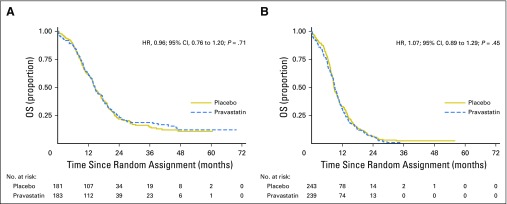
Purpose Treating small-cell lung cancer (SCLC) remains a therapeutic challenge. Experimental studies show that statins exert additive effects with agents, such as cisplatin, to impair tumor growth, and observational studies suggest that statins combined with anticancer therapies delay relapse and prolong life in several cancer types. To our knowledge, we report the first large, randomized, placebo-controlled, double-blind trial of a statin with standard-of-care for patients with cancer, specifically SCLC. Patients and Methods Patients with confirmed SCLC (limited or extensive disease) and performance status 0 to 3 were randomly assigned to receive daily pravastatin 40 mg or placebo, combined with up to six cycles of etoposide plus cisplatin or carboplatin every 3 weeks, until disease progression or intolerable toxicity. Primary end point was overall survival (OS), and secondary end points were progression-free survival (PFS), response rate, and toxicity. Results Eight hundred forty-six patients from 91 United Kingdom hospitals were recruited. The median age of recruited patients was 64 years of age, 43% had limited disease, and 57% had extensive disease. There were 758 deaths and 787 PFS events. No benefit was found for pravastatin, either in all patients or in several subgroups. For pravastatin versus placebo, the 2-year OS rate was 13.2% (95% CI, 10.0 to 16.7) versus 14.1% (95% CI, 10.9 to 17.7), respectively, with a hazard ratio of 1.01 (95% CI, 0.88 to 1.16; P = .90. The median OS was 10.7 months v 10.6 months, respectively. The median PFS was 7.7 months v 7.3 months, respectively. The median OS (pravastatin v placebo) was 14.6 months in both groups for limited disease and 9.1 months versus 8.8 months, respectively, for extensive disease. Adverse events were similar between groups. Conclusion Pravastatin 40 mg combined with standard SCLC therapy, although safe, does not benefit patients. Our conclusions are the same as those found in all four much smaller, randomized, placebo-controlled trials specifically designed to evaluate statin therapy in patients with cancer.
目的 治疗小细胞肺癌(SCLC)仍然是一项治疗挑战。实验研究表明,他汀类药物与顺铂等药物发挥协同作用以抑制肿瘤生长,观察性研究表明,他汀类药物与抗癌疗法联合使用可延缓多种癌症类型的复发并延长生存期。据我们所知,我们报告了第一项针对癌症患者,特别是SCLC患者,使用他汀类药物与标准治疗方案进行的大型、随机、安慰剂对照、双盲试验。
患者与方法 确诊为SCLC(局限期或广泛期疾病)且体力状况为0至3级的患者被随机分配接受每日40毫克普伐他汀或安慰剂治疗,每3周联合进行多达六个周期的依托泊苷加顺铂或卡铂治疗,直至疾病进展或出现无法耐受的毒性。主要终点是总生存期(OS),次要终点是无进展生存期(PFS)、缓解率和毒性。
结果 来自英国91家医院的846名患者入组。入组患者的中位年龄为64岁,43%为局限期疾病,57%为广泛期疾病。有758例死亡和787例PFS事件。在所有患者或几个亚组中均未发现普伐他汀有获益。普伐他汀组与安慰剂组相比,2年OS率分别为13.2%(95%CI,10.0至16.7)和14.1%(95%CI,10.9至17.7),风险比为1.01(95%CI,0.88至1.16;P = 0.90)。中位OS分别为10.7个月和10.6个月。中位PFS分别为7.7个月和7.3个月。局限期疾病两组的中位OS(普伐他汀组与安慰剂组)均为14.6个月,广泛期疾病分别为9.1个月和8.8个月。两组不良事件相似。
结论 40毫克普伐他汀联合标准SCLC治疗虽然安全,但对患者并无益处。我们的结论与另外四项规模小得多的、专门设计用于评估癌症患者他汀类药物治疗的随机、安慰剂对照试验的结果相同。