Fuller Brian M, Ferguson Ian T, Mohr Nicholas M, Drewry Anne M, Palmer Christopher, Wessman Brian T, Ablordeppey Enyo, Keeperman Jacob, Stephens Robert J, Briscoe Cristopher C, Kolomiets Angelina A, Hotchkiss Richard S, Kollef Marin H
Department of Emergency Medicine, Washington University School of Medicine in St. Louis, St. Louis, MO; Department of Anesthesiology, Division of Critical Care Medicine, Washington University School of Medicine in St. Louis, St. Louis, MO.
School of Medicine and Medical Science, University College Dublin, Dublin, Ireland.
Ann Emerg Med. 2017 Sep;70(3):406-418.e4. doi: 10.1016/j.annemergmed.2017.01.013. Epub 2017 Mar 2.
We evaluated the efficacy of an emergency department (ED)-based lung-protective mechanical ventilation protocol for the prevention of pulmonary complications.
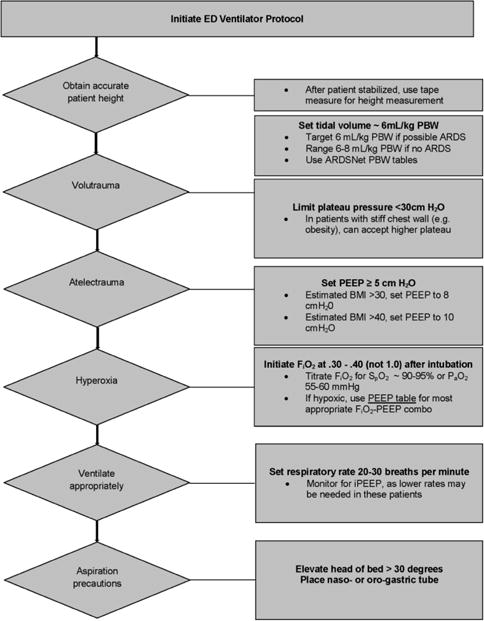
This was a quasi-experimental, before-after study that consisted of a preintervention period, a run-in period of approximately 6 months, and a prospective intervention period. The intervention was a multifaceted ED-based mechanical ventilator protocol targeting lung-protective tidal volume, appropriate setting of positive end-expiratory pressure, rapid oxygen weaning, and head-of-bed elevation. A propensity score-matched analysis was used to evaluate the primary outcome, which was the composite incidence of acute respiratory distress syndrome and ventilator-associated conditions.
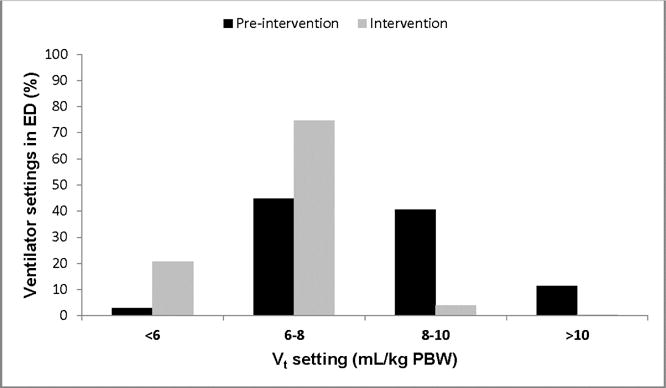
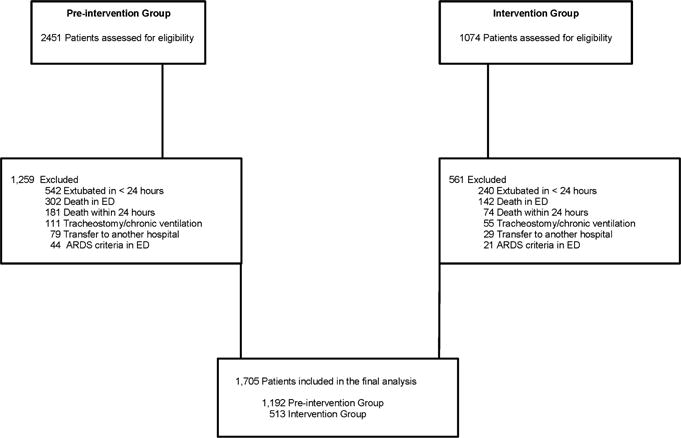
A total of 1,192 patients in the preintervention group and 513 patients in the intervention group were included. Lung-protective ventilation increased by 48.4% in the intervention group. In the propensity score-matched analysis (n=490 in each group), the primary outcome occurred in 71 patients (14.5%) in the preintervention group compared with 36 patients (7.4%) in the intervention group (adjusted odds ratio 0.47; 95% confidence interval [CI] 0.31 to 0.71). There was an increase in ventilator-free days (mean difference 3.7; 95% CI 2.3 to 5.1), ICU-free days (mean difference 2.4; 95% CI 1.0 to 3.7), and hospital-free days (mean difference 2.4; 95% CI 1.2 to 3.6) associated with the intervention. The mortality rate was 34.1% in the preintervention group and 19.6% in the intervention group (adjusted odds ratio 0.47; 95% CI 0.35 to 0.63).
Implementing a mechanical ventilator protocol in the ED is feasible and is associated with significant improvements in the delivery of safe mechanical ventilation and clinical outcome.
我们评估了基于急诊科(ED)的肺保护性机械通气方案预防肺部并发症的疗效。
这是一项准实验性的前后对照研究,包括干预前期、约6个月的导入期和前瞻性干预期。干预措施是基于急诊科的多方面机械通气方案,目标是肺保护性潮气量、呼气末正压的适当设置、快速撤氧以及床头抬高。采用倾向评分匹配分析来评估主要结局,即急性呼吸窘迫综合征和呼吸机相关病症的综合发生率。
干预前期组纳入1192例患者,干预组纳入513例患者。干预组肺保护性通气增加了48.4%。在倾向评分匹配分析中(每组n = 490),干预前期组71例患者(14.5%)出现主要结局,而干预组为36例患者(7.4%)(调整优势比0.47;95%置信区间[CI] 0.31至0.71)。干预措施使无呼吸机天数(平均差异3.7;95% CI 2.3至5.1)、无ICU天数(平均差异2.4;95% CI 1.0至3.7)和无住院天数(平均差异2.4;95% CI 1.2至3.6)均有所增加。干预前期组死亡率为34.1%,干预组为19.6%(调整优势比0.47;95% CI 0.35至0.63)。
在急诊科实施机械通气方案是可行的,并且与安全机械通气的实施及临床结局的显著改善相关。