Middleton Addie, Zhou Jie, Ottenbacher Kenneth J, Goodwin James S
Division of Rehabilitation Sciences, University of Texas Medical Branch, Galveston, Texas.
Sealy Center on Aging, University of Texas Medical Branch, Galveston, Texas.
J Am Geriatr Soc. 2017 Jun;65(6):1206-1213. doi: 10.1111/jgs.14760. Epub 2017 Mar 6.
Hospitalization in community-dwelling elderly is often accompanied by functional loss, increasing the risk for continued functional decline and future institutionalization. The primary objective of our study was to examine the hospital-level variation in rates of new institutionalizations among Medicare beneficiaries.
Retrospective cohort study.
Hospitals and nursing homes.
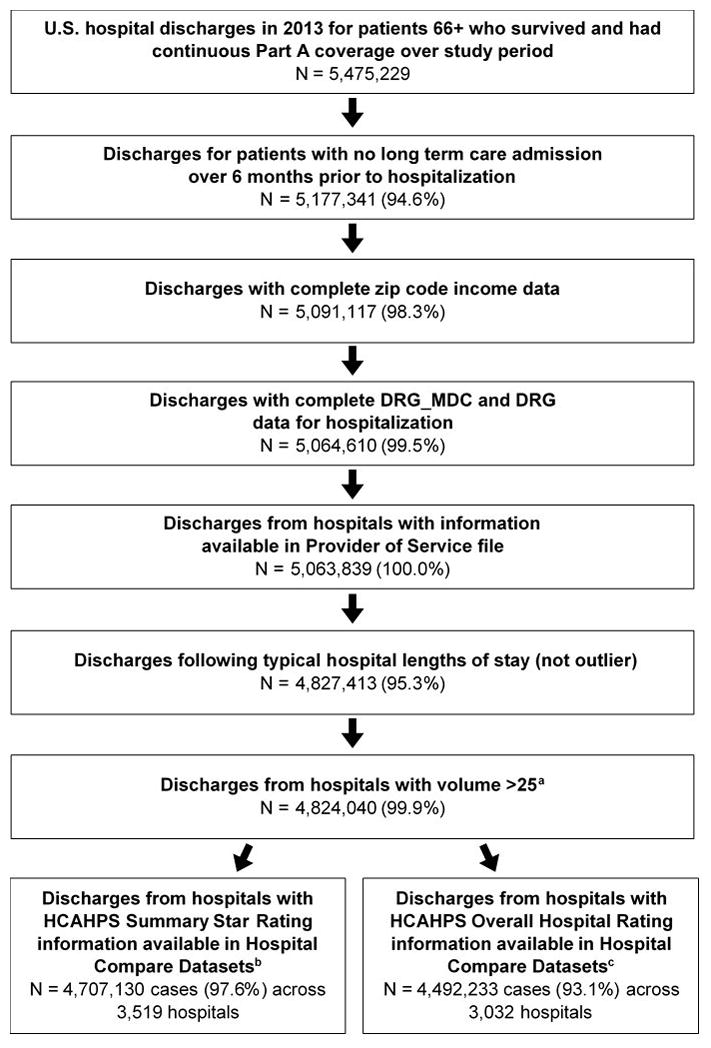
Medicare fee-for-service beneficiaries discharged from 4,469 hospitals in 2013 (N = 4,824,040).
New institutionalization, defined as new long term care nursing home residence (not skilled nursing facility) of at least 90 days duration within 6 months of hospital discharge.
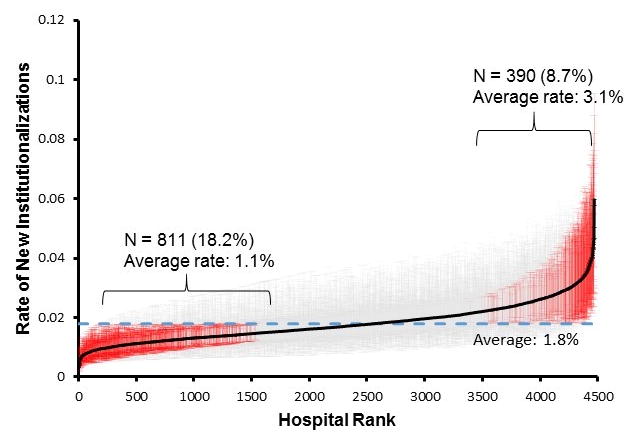
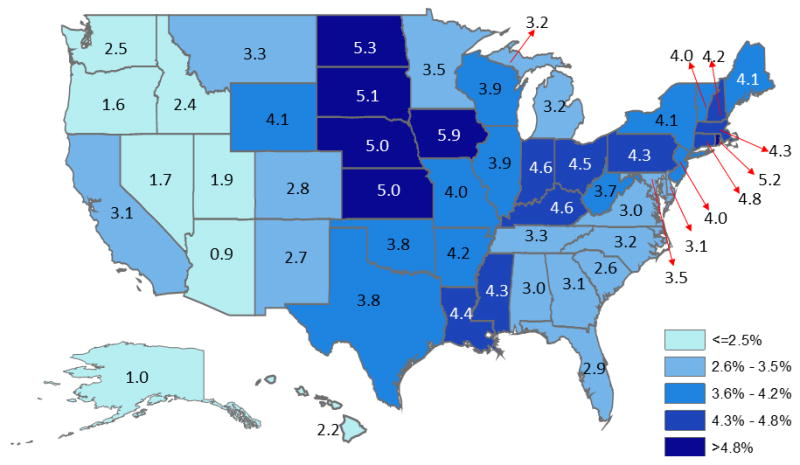
The overall observed rate of new institutionalizations was 3.6% (N = 173,998). Older age, white race, Medicaid eligibility, longer hospitalization, and having a skilled nursing facility stay over the 6 months before hospitalization were associated with higher adjusted odds. Observed rates ranged from 0.9% to 5.9% across states. The variation in rates attributable to the hospital after adjusting for case-mix and state was 5.1%. Odds were higher for patients treated in smaller (OR = 1.36, 95% CI: 1.27-1.45, ≤50 vs >500 beds), government owned (OR = 1.15, 95% CI: 1.09-1.21 compared to for-profit), limited medical school affiliation (OR = 1.13, 95% CI: 1.07-1.19 compared to major) hospitals and lower for patients treated in urban hospitals (OR = 0.79, 95% CI: 0.76-0.82 compared to rural). Higher Summary Star ratings (OR = 0.75, 95% CI: 0.67-0.93, five vs one stars) and Overall Hospital Rating (OR = 0.62, 95% CI: 0.57-0.67, ratings of 9-10 vs 0) were associated with lower odds of institutionalization.
Hospitalization may be a critical period for preventing future institutionalization among elderly patients. The variation in rates across hospitals and its association with hospital quality ratings suggest some of these institutionalizations are avoidable and may represent targets for care improvement.
社区居住老年人住院常伴有功能丧失,增加了功能持续衰退和未来入住养老机构的风险。我们研究的主要目的是调查医疗保险受益人中新增养老机构入住率在医院层面的差异。
回顾性队列研究。
医院和养老院。
2013年从4469家医院出院的医疗保险按服务收费受益人(N = 4,824,040)。
新增养老机构入住,定义为出院后6个月内新入住长期护理养老院(非专业护理机构)至少90天。
新增养老机构入住的总体观察率为3.6%(N = 173,998)。年龄较大、白人种族、符合医疗补助资格、住院时间较长以及住院前6个月内曾入住专业护理机构与调整后的较高几率相关。各州的观察率范围为0.9%至5.9%。在调整病例组合和州因素后,医院层面的差异率为5.1%。在规模较小的医院(床位≤50张与>500张相比,比值比=1.36,95%置信区间:1.27 - 1.45)、政府所有的医院(与营利性医院相比,比值比=1.15,95%置信区间:1.09 - 1.21)、医学院校附属关系有限的医院(与主要附属关系的医院相比,比值比=1.13,95%置信区间:1.07 - 1.19)接受治疗的患者几率较高,而在城市医院接受治疗的患者几率较低(与农村医院相比,比值比=0.79,95%置信区间:0.76 - 0.82)。较高的综合星级评分(五星与一星相比,比值比=0.75,95%置信区间:0.67 - 0.93)和医院总体评分(评分9 - 10分与0分相比,比值比=0.62,95%置信区间:0.57 - 0.67)与较低的入住养老机构几率相关。
住院可能是预防老年患者未来入住养老机构的关键时期。医院间的差异率及其与医院质量评分的关联表明,其中一些入住情况是可以避免的,可能是改善护理的目标。