Raffetti Elena, Donato Francesco, Casari Salvatore, Castelnuovo Filippo, Sighinolfi Laura, Bandera Alessandra, Maggiolo Franco, Ladisa Nicoletta, di Pietro Massimo, Fornabaio Chiara, Digiambenedetto Simona, Quiros-Roldan Eugenia
Unit of Hygiene, Epidemiology and Public Health, Department of Medical and Surgical Specialties, Radiological Sciences and Public Health, University of Brescia, Viale Europa 11, 25123, Brescia, Italy.
University Division of Infectious and Tropical Diseases, University of Brescia, Brescia, Italy.
BMC Infect Dis. 2017 Mar 7;17(1):193. doi: 10.1186/s12879-017-2280-5.
Two biomarkers, the neutrophil to lymphocyte ratio (NLR) and platelet to lymphocyte ratio (PLR), have been shown to be indicative of systemic inflammation and predictive of mortality in general population. We aimed to assess the association of NLR and PLR, with risk of death in HIV-infected subjects when also taking account of HIV-related factors.
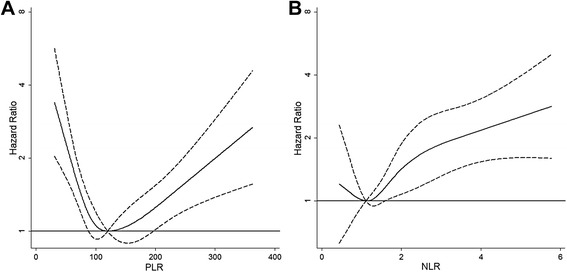
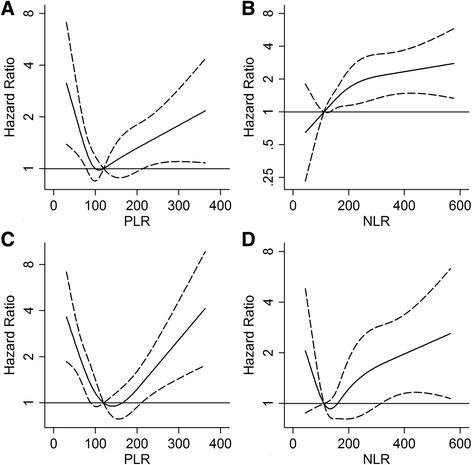
We conducted a multicenter Italian cohort study from 2000 to 2012 including HIV-infected subjects naïve at antiretroviral treatment. The associations of NLR and PLR with all-cause mortality were tested by univariate and multivariate analyses using both time independent and dependent Cox proportional hazard models. We also fitted models with a cubic-spline for PLR and NLR to evaluate the possible non-linear relationship between biomarkers values and risk of death.
Eight-thousand and two hundred thirty patients (73.1% males) with a mean age of 38.4 years (SD 10.1) were enrolled. During a median follow-up of 3.9 years, 539 patients died. PLR < 100 and ≥ 200, as compared to PLR of 100-200, and NLR ≥ 2, as compared to < 2, were associated with risk of death at both univariate and multivariate analyses. Using multivariate models with restricted cubic-splines, we found a linear relationship of increasing risk of death with increasing values for NRL over 1.1, and an U-shape curve for PLR, with higher mortality risk for values higher or lower than 120.
Our data suggest that NLR and PLR can reflect the severity of the underlying systemic disturbance of the inflammatory process and coagulation leading to augmented mortality in HIV positive subjects.
中性粒细胞与淋巴细胞比值(NLR)和血小板与淋巴细胞比值(PLR)这两种生物标志物已被证明可指示全身炎症,并能预测普通人群的死亡率。我们旨在评估NLR和PLR与HIV感染患者死亡风险之间的关联,同时考虑与HIV相关的因素。
我们在2000年至2012年期间开展了一项意大利多中心队列研究,纳入初治抗逆转录病毒治疗的HIV感染患者。使用时间独立和依赖的Cox比例风险模型,通过单变量和多变量分析来检验NLR和PLR与全因死亡率之间的关联。我们还对PLR和NLR采用三次样条拟合模型,以评估生物标志物值与死亡风险之间可能存在的非线性关系。
共纳入8230例患者(73.1%为男性),平均年龄38.4岁(标准差10.1)。在中位随访3.9年期间,539例患者死亡。单变量和多变量分析均显示,与PLR为100 - 200相比,PLR < 100和≥200,以及与NLR < 2相比,NLR≥2均与死亡风险相关。使用带有受限三次样条的多变量模型,我们发现NLR超过1.1时,死亡风险随其值增加呈线性关系,而PLR呈U形曲线,PLR值高于或低于120时死亡风险更高。
我们的数据表明,NLR和PLR可反映潜在的全身炎症和凝血紊乱的严重程度,这会导致HIV阳性患者死亡率增加。