Darling Jeremy D, McCallum John C, Soden Peter A, Korepta Lindsey, Guzman Raul J, Wyers Mark C, Hamdan Allen D, Schermerhorn Marc L
Division of Vascular and Endovascular Surgery, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, Mass.
Michigan State University College of Human Medicine, East Lansing, Mich.
J Vasc Surg. 2017 Aug;66(2):466-475. doi: 10.1016/j.jvs.2017.01.024. Epub 2017 Mar 6.
Long-term results comparing percutaneous transluminal angioplasty with or without stenting (PTA/S) and open surgical bypass for chronic limb-threatening ischemia (CLTI) in patients who have had no prior intervention are lacking.
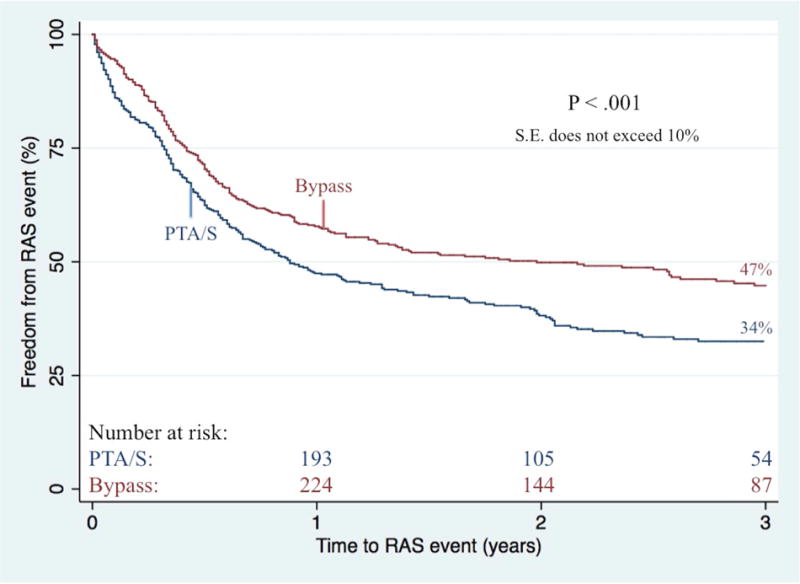
All patients undergoing a first-time lower extremity revascularization for CLTI by vascular surgeons at our institution from 2005 to 2014 were retrospectively reviewed. Outcomes included perioperative complications, wound healing, restenosis, primary patency, reintervention, major amputation, RAS events (ie, reintervention, major amputation, or stenosis), and mortality. Outcomes were evaluated using χ, Kaplan-Meier, and Cox regression analyses.
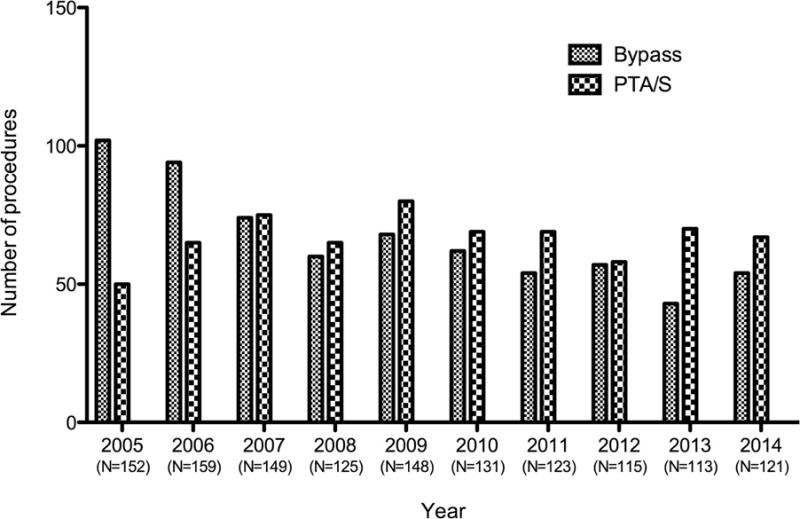
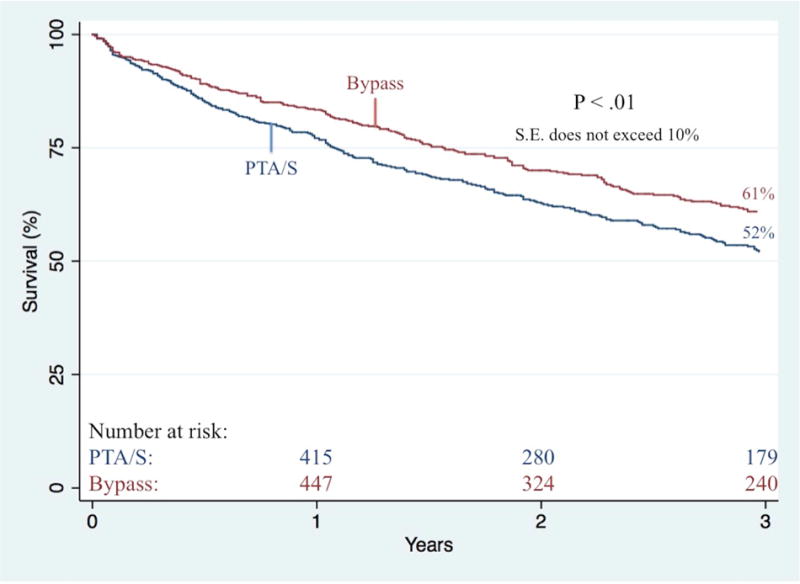
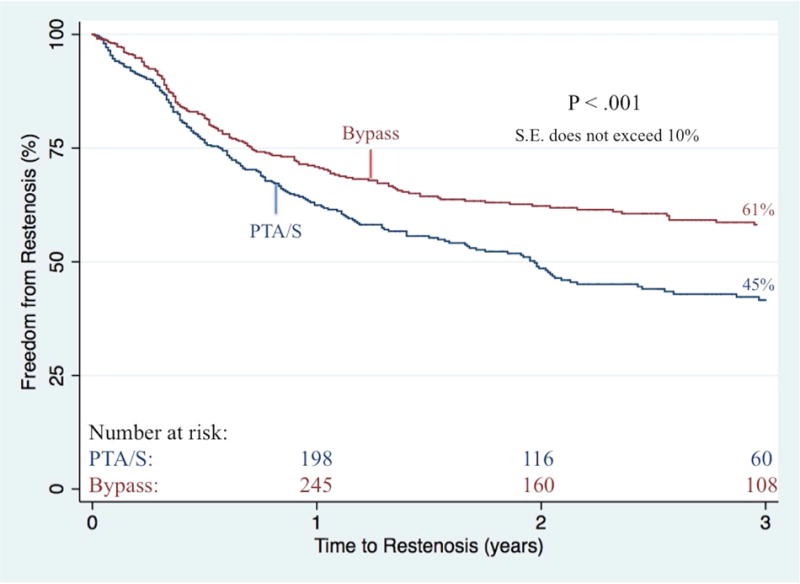
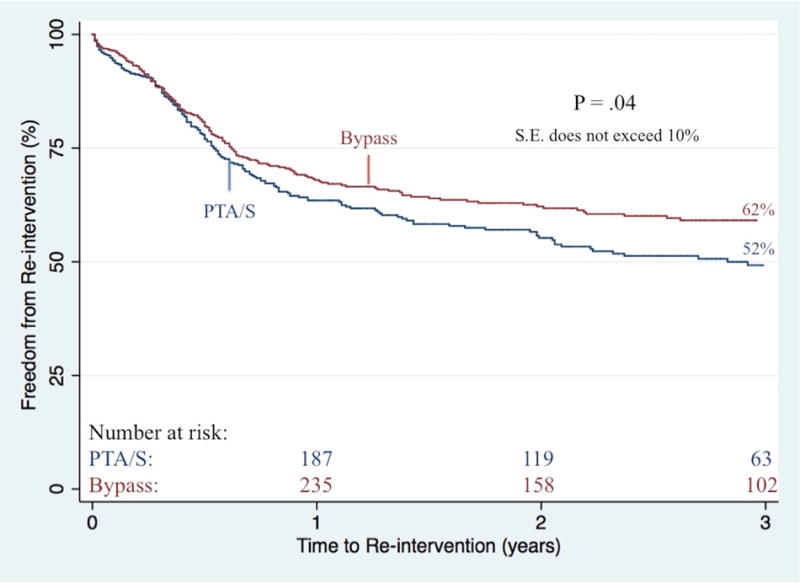
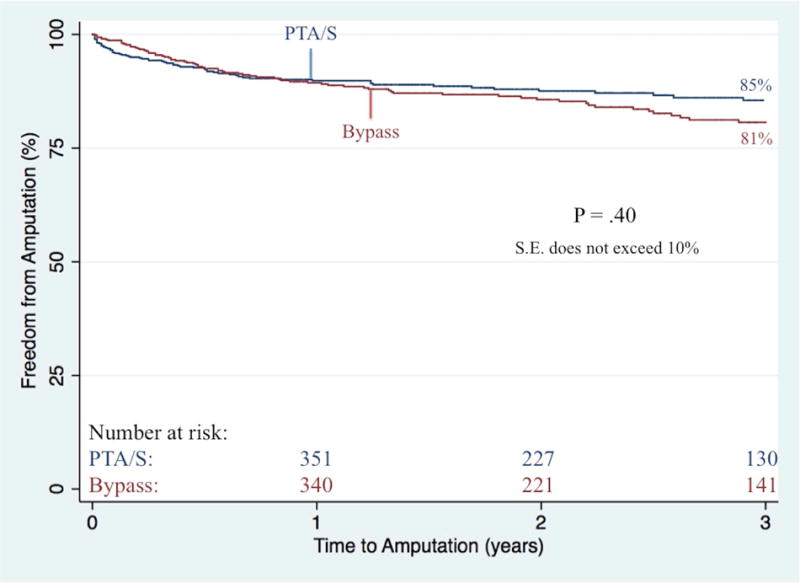
Of the 2869 total lower extremity revascularizations performed between 2005 and 2014, there were 1336 that fit our criteria of a first-time lower extremity intervention for CLTI (668 bypass procedures and 668 PTA/S procedures). Bypass patients were younger (71 vs 72 years; P = .02) and more often male (62% vs 56%; P < .02). Total mean hospital length of stay (LOS) was significantly longer after a first-time bypass (10 vs 8 days; P < .001), as were mean preoperative LOS (4 vs 3 days; P < .01) and postoperative LOS (7 vs 5 days; P < .001). There was no difference in perioperative mortality (3% vs 3%; P = .63). Surgical site infection occurred in 10% of bypass patients. Freedom from reintervention was significantly higher in patients undergoing a first-time bypass procedure (62% vs 52% at 3 years; P = .04), as was freedom from restenosis (61% vs 45% at 3 years; P < .001). Complete wound healing at 6-month follow-up was significantly better after an initial bypass (43% vs 36%; P < .01). A Cox regression model of all patients showed that reintervention was predicted by a first-time PTA/S (hazard ratio, 1.6; 95% confidence interval, 1.3-2.1) and both preoperative femoropopliteal TransAtlantic Inter-Society Consensus (TASC) C and TASC D lesions (2.0 [1.3-3.1] and 1.8 [1.3-2.7], respectively). Major amputation among all patients was predicted by an initial presentation of gangrene (2.5 [1.3-5.0]), dialysis dependence (1.9 [1.3-2.9]), diabetes (2.0 [1.1-3.8]), and preoperative femoropopliteal TASC D lesions (2.1 [1.1-4.0]) and was not predicted by procedure type.
In this retrospective analysis, bypass for the primary treatment of CLTI showed improved 6-month wound healing, higher freedom from restenosis, improved patency rates, significantly fewer reinterventions, and higher survival than PTA/S within 3 years; however, a bypass-first approach was associated with increased total hospital LOS and wound infection. Perioperative mortality and amputation rates were similar between procedure types.
对于既往未接受过干预的慢性肢体威胁性缺血(CLTI)患者,比较经皮腔内血管成形术(无论是否置入支架,即PTA/S)与开放性手术旁路移植术的长期结果尚缺乏相关研究。
对2005年至2014年期间在我院血管外科首次接受CLTI下肢血运重建术的所有患者进行回顾性分析。观察指标包括围手术期并发症、伤口愈合情况、再狭窄、原发性通畅率、再次干预、大截肢、RAS事件(即再次干预、大截肢或狭窄)以及死亡率。采用χ²检验、Kaplan-Meier法和Cox回归分析对观察指标进行评估。
在2005年至2014年期间共进行的2869例下肢血运重建术中,有1336例符合我们对CLTI首次下肢干预的标准(668例旁路移植术和668例PTA/S手术)。接受旁路移植术的患者更年轻(71岁对72岁;P = 0.02),男性比例更高(62%对56%;P < 0.02)。首次旁路移植术后总的平均住院时间(LOS)显著更长(10天对8天;P < 0.001),术前平均LOS(4天对3天;P < 0.01)和术后LOS(7天对5天;P < 0.001)也是如此。围手术期死亡率无差异(3%对3%;P = 0.63)。10%的旁路移植术患者发生手术部位感染。首次接受旁路移植术的患者再次干预的自由度显著更高(3年时为62%对52%;P = 0.04),无再狭窄的自由度也是如此(3年时为61%对45%;P < 0.001)。初次旁路移植术后6个月随访时完全伤口愈合情况显著更好(43%对36%;P < 0.01)。对所有患者的Cox回归模型显示,首次PTA/S(风险比,1.6;95%置信区间,1.3 - 2.1)以及术前股腘动脉跨大西洋两岸血管外科学会共识(TASC)C型和T型病变(分别为2.0 [1.3 - 3.1]和1.8 [1.3 - 2.7])可预测再次干预。所有患者中的大截肢可通过坏疽的初始表现(2.5 [1.3 - 5.0])、透析依赖(1.9 [1.3 - 2.9])、糖尿病(2.0 [1.1 - 3.8])以及术前股腘动脉TASC D型病变(2.1 [1.1 - 4.0])进行预测,且与手术类型无关。
在这项回顾性分析中,CLTI的初次治疗采用旁路移植术与PTA/S相比,6个月时伤口愈合情况改善、无再狭窄自由度更高、通畅率提高、再次干预显著减少且3年内生存率更高;然而,先行旁路移植术的方法与总住院LOS增加和伤口感染相关。不同手术类型的围手术期死亡率和截肢率相似。