Kerckhove Nicolas, Collin Aurore, Condé Sakahlé, Chaleteix Carine, Pezet Denis, Balayssac David
INSERM U1107, NEURO-DOL, CHU Clermont-Ferrand, Délégation à la Recherche Clinique et à l'Innovation, Université Clermont Auvergne Clermont-Ferrand, France.
INSERM U1107, NEURO-DOL, Université Clermont Auvergne Clermont-Ferrand, France.
Front Pharmacol. 2017 Feb 24;8:86. doi: 10.3389/fphar.2017.00086. eCollection 2017.
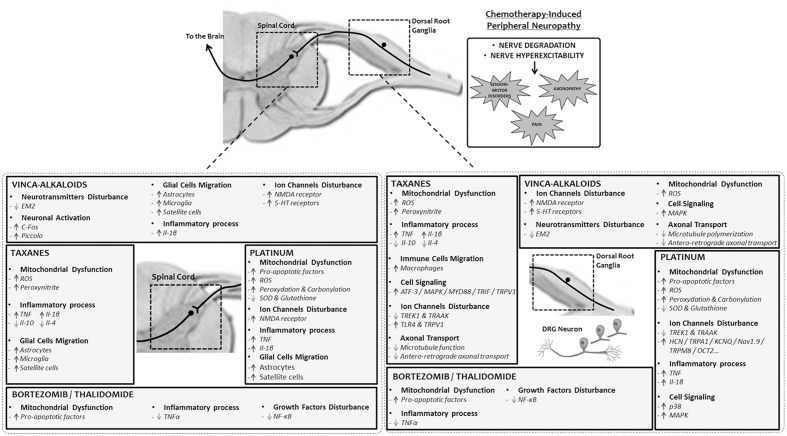
Neurotoxic anticancer drugs, such as platinum-based anticancer drugs, taxanes, vinca alkaloids, and proteasome/angiogenesis inhibitors are responsible for chemotherapy-induced peripheral neuropathy (CIPN). The health consequences of CIPN remain worrying as it is associated with several comorbidities and affects a specific population of patients already impacted by cancer, a strong driver for declines in older adults. The purpose of this review is to present a comprehensive overview of the long-term effects of CIPN in cancer patients and survivors. Pathophysiological mechanisms and risk factors are also presented. Neurotoxic mechanisms leading to CIPNs are not yet fully understood but involve neuronopathy and/or axonopathy, mainly associated with DNA damage, oxidative stress, mitochondria toxicity, and ion channel remodeling in the neurons of the peripheral nervous system. Classical symptoms of CIPNs are peripheral neuropathy with a "stocking and glove" distribution characterized by sensory loss, paresthesia, dysesthesia and numbness, sometimes associated with neuropathic pain in the most serious cases. Several risk factors can promote CIPN as a function of the anticancer drug considered, such as cumulative dose, treatment duration, history of neuropathy, combination of therapies and genetic polymorphisms. CIPNs are frequent in cancer patients with an overall incidence of approximately 38% (possibly up to 90% of patients treated with oxaliplatin). Finally, the long-term reversibility of these CIPNs remain questionable, notably in the case of platinum-based anticancer drugs and taxanes, for which CIPN may last several years after the end of anticancer chemotherapies. These long-term effects are associated with comorbidities such as depression, insomnia, falls and decreases of health-related quality of life in cancer patients and survivors. However, it is noteworthy that these long-term effects remain poorly studied, and only limited data are available such as in the case of bortezomib and thalidomide-induced peripheral neuropathy.
神经毒性抗癌药物,如铂类抗癌药物、紫杉烷类、长春花生物碱以及蛋白酶体/血管生成抑制剂,是化疗引起的周围神经病变(CIPN)的病因。CIPN对健康造成的后果仍然令人担忧,因为它与多种合并症相关,且影响着已经受到癌症影响的特定患者群体,而癌症是导致老年人健康状况下降的一个重要因素。本综述的目的是全面概述CIPN对癌症患者和幸存者的长期影响。同时还介绍了病理生理机制和危险因素。导致CIPN的神经毒性机制尚未完全明确,但涉及神经元病变和/或轴索性病变,主要与外周神经系统神经元中的DNA损伤、氧化应激、线粒体毒性以及离子通道重塑有关。CIPN的典型症状是呈“袜套样和手套样”分布的周围神经病变,其特征为感觉丧失、感觉异常、感觉障碍和麻木,在最严重的情况下有时还伴有神经性疼痛。根据所使用的抗癌药物不同,有几种危险因素可促使CIPN的发生,如累积剂量、治疗持续时间、神经病变史、联合治疗以及基因多态性。CIPN在癌症患者中很常见,总体发生率约为38%(使用奥沙利铂治疗的患者可能高达90%)。最后,这些CIPN的长期可逆性仍然存疑,尤其是对于铂类抗癌药物和紫杉烷类药物而言,CIPN可能在抗癌化疗结束后持续数年。这些长期影响与诸如抑郁症、失眠、跌倒以及癌症患者和幸存者健康相关生活质量下降等合并症有关。然而,值得注意的是,这些长期影响的研究仍然很少,仅有有限的数据,如硼替佐米和沙利度胺引起的周围神经病变的情况。