Schroeder Daniel C, Guschlbauer Maria, Maul Alexandra C, Cremer Daniel A, Becker Ingrid, de la Puente Bethencourt David, Paal Peter, Padosch Stephan A, Wetsch Wolfgang A, Annecke Thorsten, Böttiger Bernd W, Sterner-Kock Anja, Herff Holger
Department of Anaesthesiology and Intensive Care Medicine, University Hospital of Cologne, Kerpener Straße 62, Cologne, Germany.
Department of Experimental Medicine, University Hospital of Cologne, Cologne, Germany.
PLoS One. 2017 Mar 14;12(3):e0173229. doi: 10.1371/journal.pone.0173229. eCollection 2017.
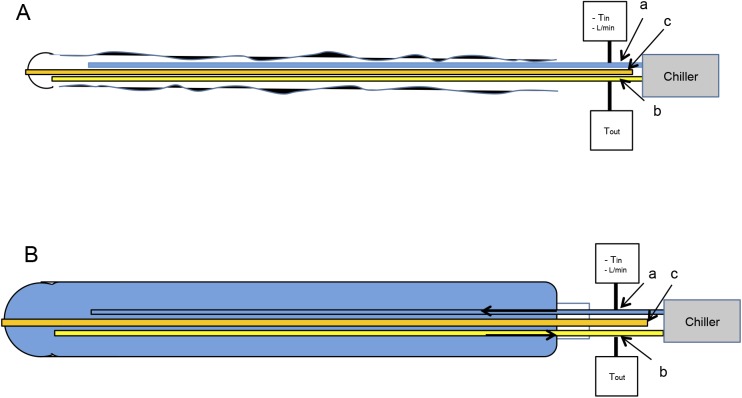
Targeted temperature management (TTM) is widely used in critical care settings for conditions including hepatic encephalopathy, hypoxic ischemic encephalopathy, meningitis, myocardial infarction, paediatric cardiac arrest, spinal cord injury, traumatic brain injury, ischemic stroke and sepsis. Furthermore, TTM is a key treatment for patients after out-of-hospital cardiac-arrest (OHCA). However, the optimal cooling method, which is quick, safe and cost-effective still remains controversial. Since the oesophagus is adjacent to heart and aorta, fast heat-convection to the central blood-stream could be achieved with a minimally invasive oesophageal heat exchanger (OHE). To date, the optimal diameter of an OHE is still unknown. While larger diameters may cause thermal- or pressure-related tissue damage after long-term exposure to the oesophageal wall, smaller diameter (e.g., gastric tubes, up to 11mm) may not provide effective cooling rates. Thus, the objective of the study was to compare OHE-diameters of 11mm (OHE11) and 14.7mm (OHE14.7) and their effects on tissue and cooling capability.
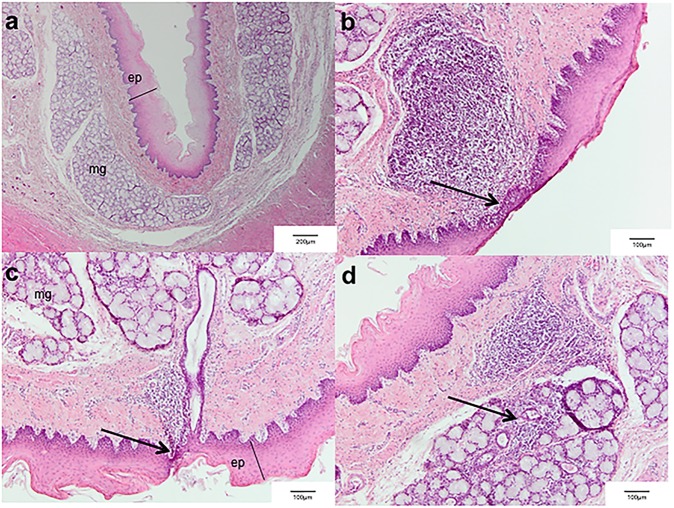
Pigs were randomized to OHE11 (N = 8) or OHE14.7 (N = 8). After cooling, pigs were maintained at 33°C for 1 hour. After 10h rewarming, oesophagi were analyzed by means of histopathology. The oesophagus of four animals from a separate study that underwent exactly the identical preparation and cooling protocol described above but received a maintenance period of 24h were used as histopathological controls.
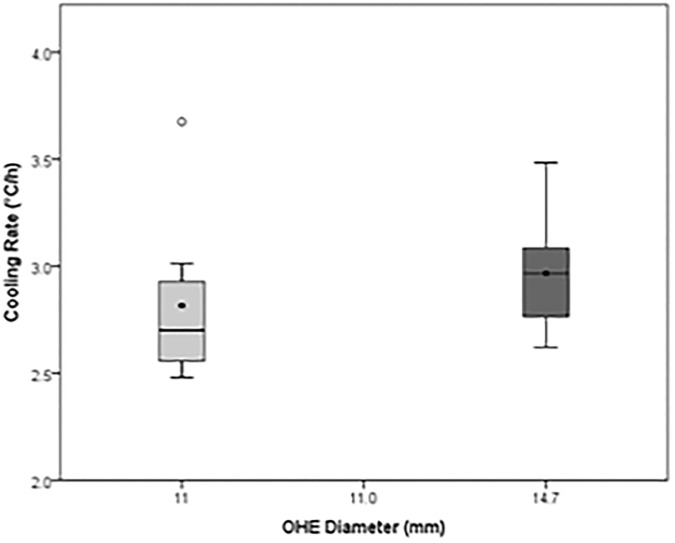
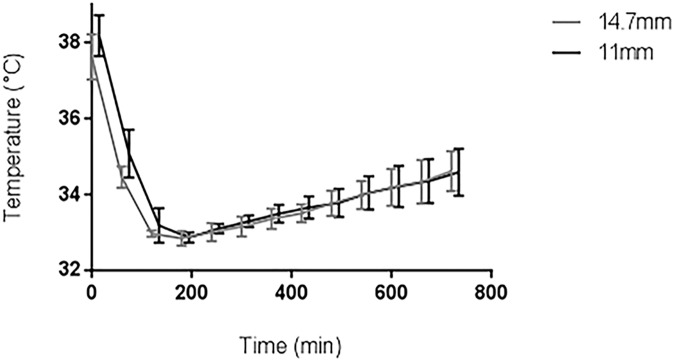
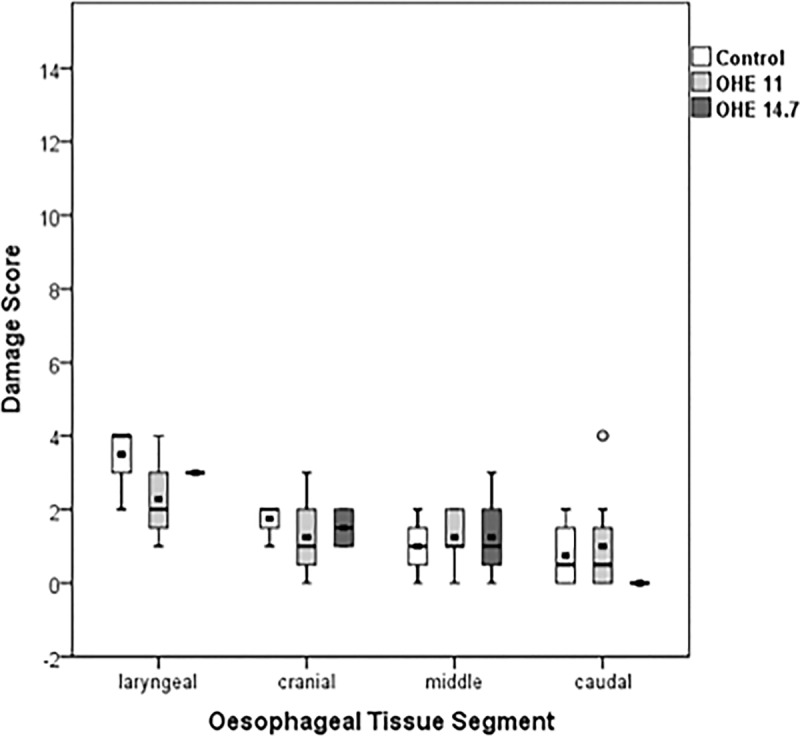
Mean cooling rates were 2.8±0.4°C°C/h (OHE11) and 3.0±0.3°C °C/h (OHE14.7; p = 0.20). Occasional mild acute inflammatory transepithelial infiltrates were found in the cranial segment of the oesophagus in all groups including controls. Deviations from target temperature were 0.1±0.4°C (OHE11) and 0±0.1°C (OHE14.7; p = 0.91). Rewarming rates were 0.19±0.07°C °C/h (OHE11) and 0.20±0.05°C °C/h (OHE14.7; p = 0.75).
OHE with diameters of 11 mm and 14.7 mm achieve effective cooling rates for TTM and did not cause any relevant oesophageal tissue damage. Both OHE demonstrated acceptable deviations from target temperature and allowed for an intended rewarming rate (0.25°C/h).
目标温度管理(TTM)广泛应用于重症监护环境,用于治疗包括肝性脑病、缺氧缺血性脑病、脑膜炎、心肌梗死、小儿心脏骤停、脊髓损伤、创伤性脑损伤、缺血性中风和脓毒症等病症。此外,TTM是院外心脏骤停(OHCA)患者的关键治疗方法。然而,快速、安全且具有成本效益的最佳降温方法仍存在争议。由于食管与心脏和主动脉相邻,使用微创食管热交换器(OHE)可实现向中心血流的快速热对流。迄今为止,OHE的最佳直径仍不清楚。虽然较大直径在长期接触食管壁后可能会导致与热或压力相关的组织损伤,但较小直径(例如胃管,最大11mm)可能无法提供有效的降温速率。因此,本研究的目的是比较11mm(OHE11)和14.7mm(OHE14.7)的OHE直径及其对组织和降温能力的影响。
将猪随机分为OHE11组(N = 8)或OHE14.7组(N = 8)。降温后,将猪维持在33°C 1小时。复温10小时后,通过组织病理学分析食管。从另一项单独研究中选取4只动物的食管,这些动物接受了与上述完全相同的准备和降温方案,但维持期为24小时,用作组织病理学对照。
平均降温速率为2.8±0.4°C/h(OHE11)和3.0±0.3°C/h(OHE14.7;p = 0.20)。在包括对照组在内的所有组中,在食管头段偶尔发现轻度急性炎症性跨上皮浸润。与目标温度的偏差为0.1±0.4°C(OHE11)和0±0.1°C(OHE14.7;p = 0.91)。复温速率为0.19±0.07°C/h(OHE11)和0.20±0.05°C/h(OHE14.7;p = 0.75)。
直径为11mm和