Santos Sherie Lou Zara, Tagai Erin K, Scheirer Mary Ann, Bowie Janice, Haider Muhiuddin, Slade Jimmie, Wang Min Qi, Holt Cheryl L
Department of Behavioral and Community Health, University of Maryland, School of Public Health, 4200 Valley Dr., 1101 E SPH Building 255, College Park, MD, 20742, USA.
Scheirer Consulting, Princeton, NJ, USA.
Implement Sci. 2017 Mar 14;12(1):36. doi: 10.1186/s13012-017-0566-z.
Use of technology is increasing in health promotion and has continued growth potential in intervention research. Guided by the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) framework, this paper reports on the adoption, reach, and implementation of Project HEAL (Health through Early Awareness and Learning)-a community-based implementation trial of a cancer educational intervention in 14 African American churches. We compare adoption, reach, and implementation at the organizational and participant level for churches in which lay peer community health advisors (CHAs) were trained using traditional classroom didactic methods compared with a new online system.
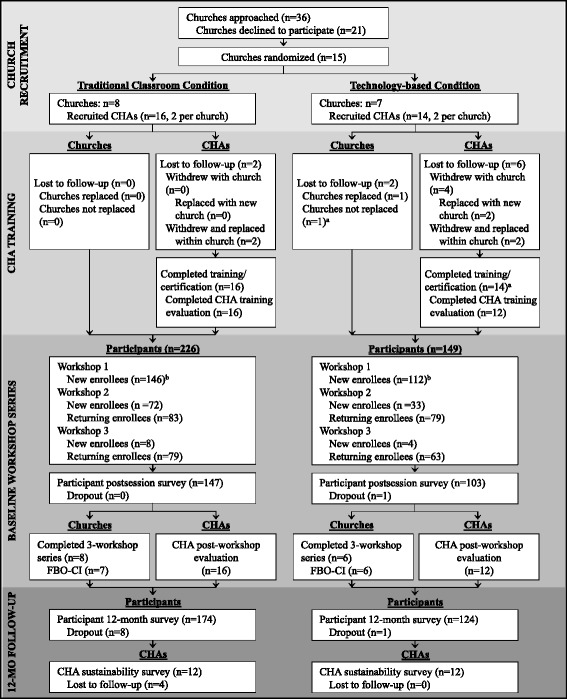
Fifteen churches were randomized to one of two study groups in which two CHAs per church were trained through either classroom ("Traditional"; n = 16 CHAs in 8 churches) or web-based ("Technology"; n = 14 CHAs in 7 churches) training methods. Once trained and certified, all CHAs conducted a series of three group educational workshops in their churches on cancer early detection (breast, prostate, and colorectal). Adoption, reach, and implementation were assessed using multiple data sources including church-level data, participant engagement in the workshops, and study staff observations of CHA performance.
The project had a 41% overall adoption rate at the church level. In terms of reach, a total of 375 participants enrolled in Project HEAL-226 participants in the Traditional group (43% reach) and 149 in the Technology group (21% reach; p < .10). Implementation was evaluated in terms of adherence, dosage, and quality. All churches fully completed the three workshops; however, the Traditional churches took somewhat longer (M = 84 days) to complete the workshop series than churches in the Technology group (M = 64 days). Other implementation outcomes were comparable between both the Traditional and Technology groups (p > .05).
Overall, the Project HEAL intervention had reasonable adoption, though reach could have been better. Implementation was strong across both study groups, suggesting the promise of using web-based methods to disseminate and implement evidence-based interventions in faith-based settings and other areas where community health educators work to eliminate health disparities.
技术在健康促进中的应用正在增加,在干预研究中具有持续的增长潜力。在“覆盖、效果、采用、实施和维持”(RE-AIM)框架的指导下,本文报告了“通过早期意识与学习促进健康”(HEAL)项目的采用、覆盖范围和实施情况——这是一项在14个非裔美国教会中开展的基于社区的癌症教育干预实施试验。我们比较了采用传统课堂教学方法培训非专业同伴社区健康顾问(CHA)的教会与采用新在线系统的教会在组织和参与者层面的采用、覆盖范围和实施情况。
15个教会被随机分配到两个研究组之一,每个教会的两名CHA通过课堂培训(“传统组”;8个教会中的16名CHA)或基于网络的培训(“技术组”;7个教会中的14名CHA)方法进行培训。一旦接受培训并获得认证,所有CHA在其教会中举办了一系列三场关于癌症早期检测(乳腺癌、前列腺癌和结直肠癌)的小组教育研讨会。采用多种数据源评估采用、覆盖范围和实施情况,包括教会层面的数据、参与者在研讨会上的参与情况以及研究人员对CHA表现的观察。
该项目在教会层面的总体采用率为41%。在覆盖范围方面,共有375名参与者参加了HEAL项目——传统组有226名参与者(覆盖率43%),技术组有149名参与者(覆盖率21%;p<0.10)。从依从性、剂量和质量方面对实施情况进行评估。所有教会都完全完成了三场研讨会;然而,传统组的教会完成研讨会系列的时间略长(平均84天),而技术组的教会完成时间为(平均64天)。传统组和技术组的其他实施结果相当(p>0.05)。
总体而言,HEAL项目干预措施的采用情况合理,尽管覆盖范围本可以更好。两个研究组的实施情况都很好,这表明在基于信仰的环境以及社区健康教育工作者致力于消除健康差距的其他领域,使用基于网络的方法传播和实施循证干预措施具有前景。