Reggiani Bonetti Luca, Lionti Simona, Domati Federica, Barresi Valeria
Luca Reggiani Bonetti, Federica Domati, Department of Laboratory Integrated Activities, Anatomic Pathology and Legal Medicine, Section of Pathology, University of Modena and Reggio Emilia, 41124 Modena, Italy.
World J Gastroenterol. 2017 Feb 28;23(8):1412-1423. doi: 10.3748/wjg.v23.i8.1412.
To clarify which factors may influence pathological tumor response and affect clinical outcomes in patients with locally advanced rectal carcinoma treated with neo-adjuvant chemoradiotherapy and surgery.
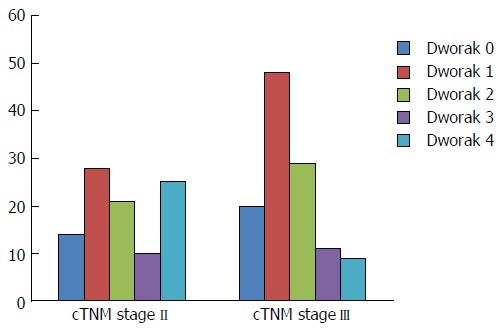
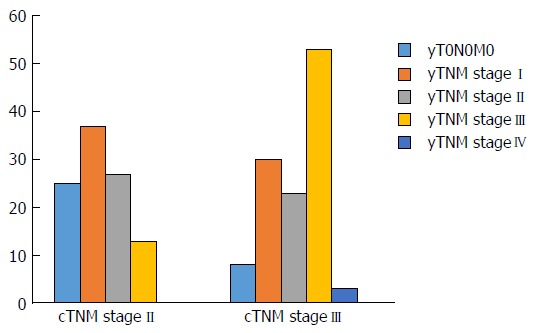
Tumor regression grade (TRG) according to the Dworak system and yTNM stage were assessed and correlated with pre-treatment clinico-pathological variables in 215 clinically locally advanced (cTNM stage II and III) rectal carcinomas. Prognostic value of all pathological and clinical factors on disease free survival (DFS) and cancer specific survival (CSS) was analyzed by Kaplan Meier and Cox-regression analyses.
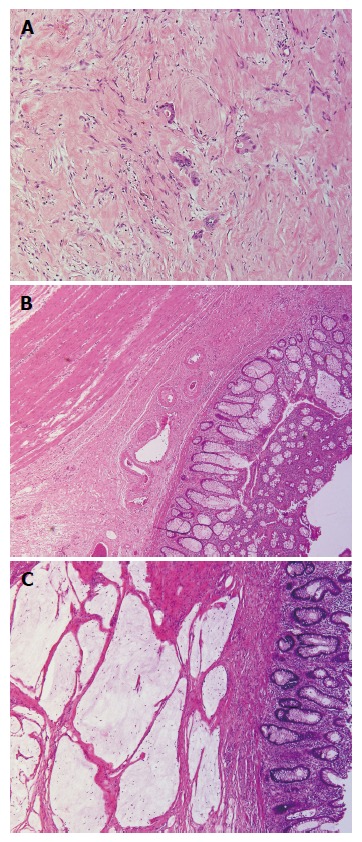
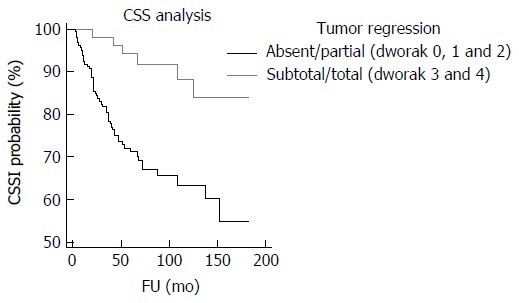
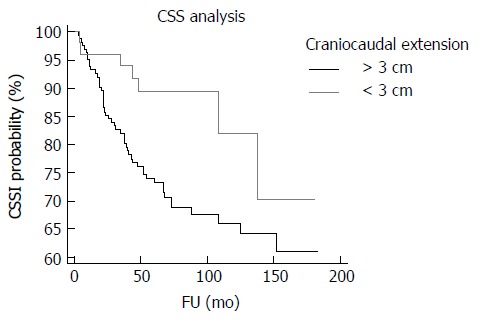
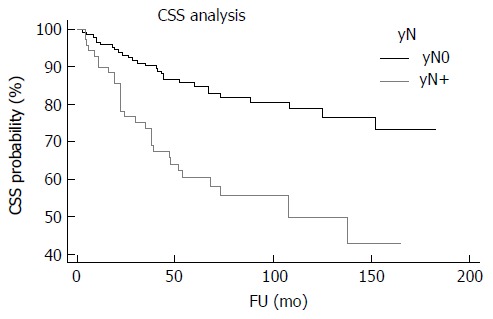
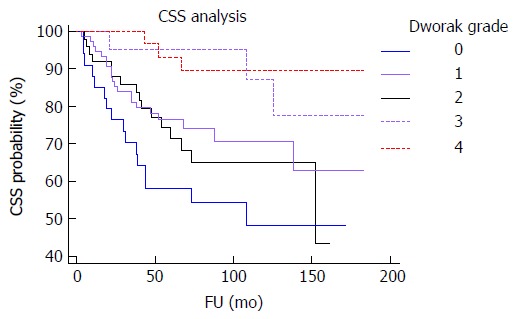
cN+ status, mucinous histotype or poor differentiation in the pre-treatment biopsy were significantly associated with lower pathological response (low Dworak grade and TNM remaining unchanged/upstaging). Cases showing acellular mucin pools in surgical specimens all had unremarkable clinical courses with no deaths or recurrences during follow-up. Dworak grade had prognostic significance for DFS and CSS. However, compared to the 5-tiered system, a simplified two-tiered grading system, in which grades 0, 1 and 2 were grouped as absent/partial regression and grades 3 and 4 were grouped as total/subtotal regression, was more reproducible and prognostically informative. The two-tiered Dworak system, yN stage, craniocaudal extension of the tumor and radial margin status were significant independent prognostic variables.
Our data suggest that caution should be applied in using a conservative approach in rectal carcinomas with cN+ status, extensive/lower involvement of the rectum and mucinous histotype or poor differentiation. Although Dworak TRG is prognostically significant, a simplified two-tiered system could be preferable. Finally, cases with acellular mucin pools should be carefully evaluated to definitely exclude residual mucinous carcinoma.
明确在接受新辅助放化疗及手术治疗的局部晚期直肠癌患者中,哪些因素可能影响肿瘤的病理反应并影响临床结局。
对215例临床局部晚期(cTNM分期为II期和III期)直肠癌患者,根据Dworak系统评估肿瘤退缩分级(TRG)及yTNM分期,并将其与治疗前临床病理变量进行关联分析。通过Kaplan-Meier法和Cox回归分析,分析所有病理和临床因素对无病生存期(DFS)和癌症特异性生存期(CSS)的预后价值。
治疗前活检中cN+状态、黏液组织学类型或低分化与较低的病理反应(低Dworak分级且TNM分期未改变/分期上升)显著相关。手术标本中显示无细胞黏液池的病例,其临床病程均无异常,随访期间无死亡或复发。Dworak分级对DFS和CSS具有预后意义。然而,与五级系统相比,一种简化的两级分级系统(其中0、1和2级归为无/部分退缩,3和4级归为完全/次全退缩)更具可重复性且预后信息更丰富。两级Dworak系统、yN分期、肿瘤的头尾延伸及切缘状态是显著的独立预后变量。
我们的数据表明,对于cN+状态、直肠广泛/低位受累、黏液组织学类型或低分化的直肠癌患者,采用保守治疗方法时应谨慎。尽管Dworak TRG具有预后意义,但简化的两级系统可能更可取。最后,对于有无细胞黏液池的病例,应仔细评估以明确排除残留黏液癌。