Liu Jin, Fan Lin, Zhu Yingbo, Yu Haotong, Xu Tianyang, Li Guodong
Department of Orthopedics, Taihu Hospital of Wuxi, Wuxi Department of Orthopedics, Shanghai Tenth People's Hospital Nan Jing Medical University, Nangjing Tongji University School of Medicine, Shanghai Department of Psychiatry, Shanghai Tenth People's Hospital, Shanghai, People's Republic of China.
Medicine (Baltimore). 2017 Mar;96(11):e6322. doi: 10.1097/MD.0000000000006322.
The aim of the study was to compare the clinical outcomes of patients undergoing all-arthroscopic (AA) or mini-open (MO) rotator cuff repair.
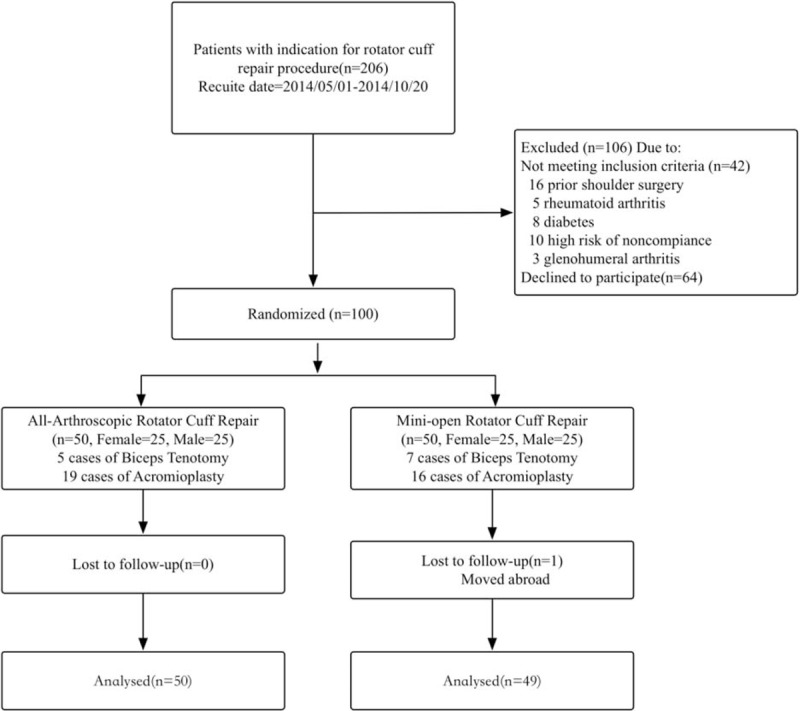
The present study evaluated 50 patients who had undergone AA repair and 50 patients who had undergone MO repair with a minimum 1-year follow-up. Every patient was asked to complete the Disabilities of the Arm, Shoulder and Hand (DASH) and visual analog scale (VAS) questionnaires. Constant-Murley score (CMS) and active ranges, forward flexion and external rotation, were also evaluated and documented. One year after surgery, ultrasound evaluation was done to determine the integrity of the rotator cuff for each patient.
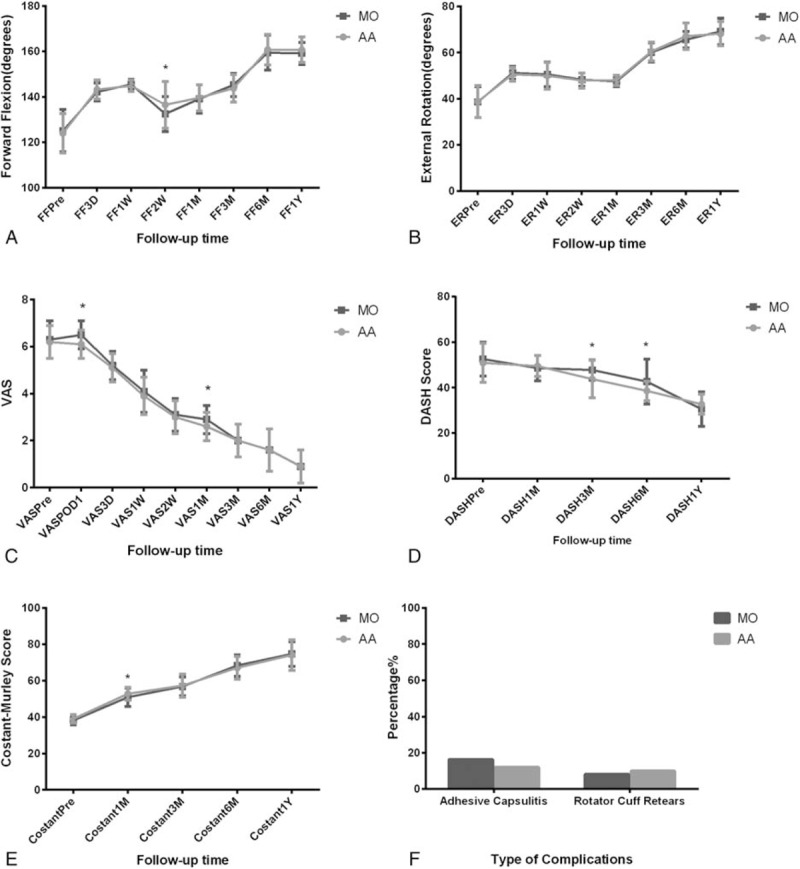
The average age of enrolled patients at the time of surgery was 53.0 years (range, 40-59 years), and average follow-up was 16.6 months (range, 12-24 months). At 2 weeks, the range of forward flexion in the AA group was larger than that in the MO group (136.5 ± 10.2 vs 132.5 ± 7.7, P = 0.03). On postoperative day 1, the VAS in the MO group was significantly higher than that in the AA group (6.5 ± 0.6 vs 6.1 ± 0.6, P < 0.01). At 1 month, the difference in VAS between both groups reappeared (2.9 ± 0.6 vs 2.6 ± 0.6, P = 0.03). At 1 month, the CMS score of patients in the AA group was higher than that in the MO group (52.8 ± 3.6 vs 50.9 ± 5.0, P = 0.03). At 3 and 6 months, the DASH score of patients in the AA group was lower than that in the MO group (43.8 ± 8.2 vs 47.8 ± 4.4, P < 0.01 and 38.6 ± 4.3 vs 42.7 ± 9.9, P < 0.01, respectively). Mean operative time was longer in the AA group compared with that in the MO group (71.9 ± 17.6 vs 64.7 ± 12.7 minutes, P < 0.01). Five patients (10.0%) in the AA group and 4 patients (8.2%) in the MO group had rotator cuff retear, and 6 patients (12.0%) in the AA group and 8 patients (16.3%) in the MO group had adhesive capsulitis by the end of follow-up. There is no significant difference between the 2 groups in the incidence of complications. We also found that joint exercising at least 3 times per week was associated with better short- and long-term joint function recovery.
The AA approach was associated with less pain and lower DASH score as well as higher CMS score in the early recovery period. No difference was found between the 2 groups in primary and secondary outcomes in the long term, or incidence of complications such as adhesive capsulitis and rotator cuff retear. In conclusion, we consider that the AA procedure has better recovery at short-term follow-ups, while both techniques are equivalent regarding long-term outcomes.
本研究旨在比较接受全关节镜(AA)或小切口开放(MO)肩袖修复术患者的临床结局。
本研究评估了50例行AA修复术和50例行MO修复术且随访至少1年的患者。每位患者均被要求完成上肢、肩部和手部功能障碍(DASH)及视觉模拟量表(VAS)问卷。同时评估并记录Constant-Murley评分(CMS)以及主动活动范围,即前屈和外旋。术后1年,进行超声评估以确定每位患者肩袖的完整性。
入选患者手术时的平均年龄为53.0岁(范围40 - 59岁),平均随访时间为16.6个月(范围12 - 24个月)。术后2周,AA组的前屈范围大于MO组(136.5±10.2对132.5±7.7,P = 0.03)。术后第1天,MO组的VAS显著高于AA组(6.5±0.6对6.1±0.6,P < 0.01)。术后1个月,两组间VAS差异再次出现(2.9±0.6对2.6±0.6,P =
0.03)。术后1个月,AA组患者的CMS评分高于MO组(52.8±3.6对50.9±5.0,P = 0.03)。术后3个月和6个月,AA组患者的DASH评分低于MO组(43.8±8.2对47.8±4.4,P < 0.01;38.6±4.3对42.7±9.9,P < 0.01)。AA组的平均手术时间长于MO组(71.9±17.6对64.7±12.7分钟,P < 0.01)。随访结束时,AA组有5例患者(10.0%)发生肩袖再撕裂,MO组有4例患者(8.2%)发生;AA组有6例患者(12.0%)发生粘连性关节囊炎,MO组有8例患者(16.3%)发生。两组并发症发生率无显著差异。我们还发现每周至少进行3次关节锻炼与更好的短期和长期关节功能恢复相关。
AA手术方式在早期恢复阶段疼痛较轻、DASH评分较低且CMS评分较高。两组在长期的主要和次要结局方面,以及粘连性关节囊炎和肩袖再撕裂等并发症发生率方面均未发现差异。总之,我们认为AA手术在短期随访中恢复较好,而两种技术在长期结局方面相当。