Rubin David T, Dubinsky Marla C, Martino Steve, Hewett Kathleen A, Panés Julian
*Department of Medicine, Inflammatory Bowel Disease Center, The University of Chicago Medicine, Chicago, Illinois; †Susan and Leonard Feinstein Clinical IBD Center, Icahn School of Medicine at Mount Sinai, New York, New York; ‡M Health, Philadelphia, Pennsylvania; §Ogilvy CommonHealth Behavioral Insights, Parsippany, New Jersey; and ‖IDIBAPS, Hospital Clinic de Barcelona, CIBERehd, Barcelona, Spain.
Inflamm Bowel Dis. 2017 Apr;23(4):494-501. doi: 10.1097/MIB.0000000000001048.
We analyzed in-office communication between patients with ulcerative colitis (UC) and their gastroenterologists.
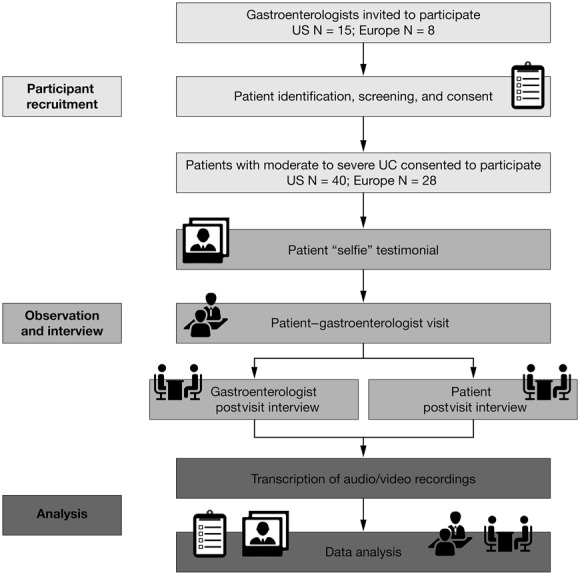
Participating gastroenterologists (United States N = 15; Europe N = 8) identified eligible patients with scheduled clinic visits. Patients (United States N = 40; Europe N = 28; ≥18 yr old; physician-defined moderately-to-severely active ulcerative colitis for approximately ≥1 yr; ≥1 flare in preceding year; prior or current therapy with 5-aminosalicylates and/or corticosteroids) consented to have their visit recorded. Follow-up interviews were conducted separately with gastroenterologists and patients. Transcripts were analyzed using sociolinguistic methods to explore quality of life (QoL) impacts, treatment goals, and attitudes to therapies.
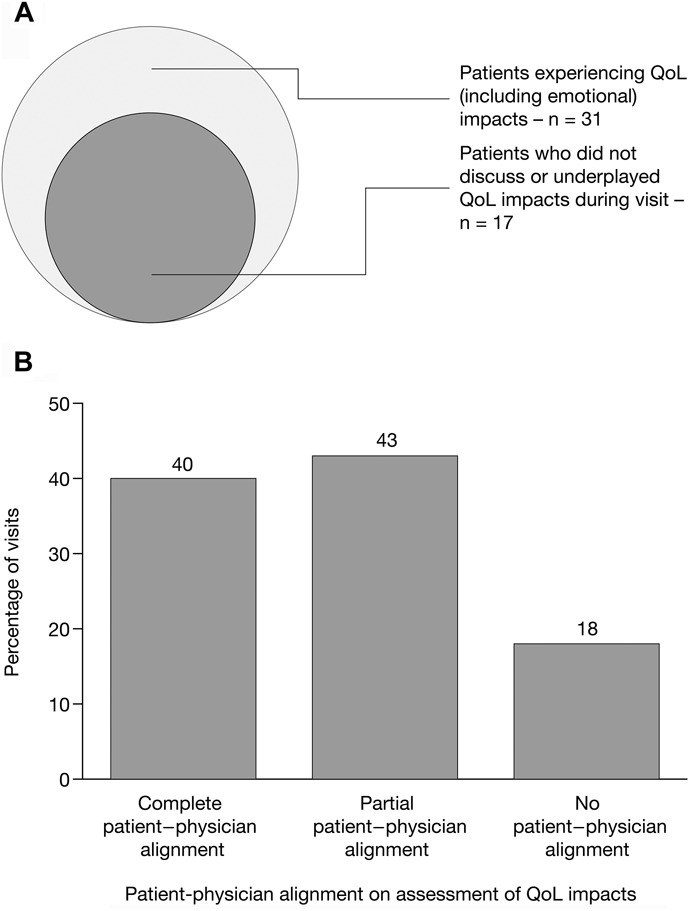
In the European and U.S. research, the trend was for patients not to discuss ulcerative colitis QoL impacts during their visits. In the U.S. research, complete patient-physician alignment on QoL impacts (patient and physician stating the same impacts) was seen in 40% of cases. Variation in treatment goals was seen between gastroenterologists and patients: 3% of U.S. patients described absence of inflammation as a treatment goal versus 25% of gastroenterologists. This goal was not always conveyed to the patient during visits. Consistent with guidelines, physicians generally framed biologic therapy as suitable for patients refractory to conventional therapies. However, although putative efficacy offered by biologic therapy is generally aligned with patients' stated treatment goals, many considered biologic therapy as more appropriate for more severe disease than theirs.
Alignment between patients and physicians on ulcerative colitis QoL impact, treatment goals, and requirement of advanced therapies is poor. New tools are needed to cover this gap.
我们分析了溃疡性结肠炎(UC)患者与其胃肠病学家在诊室的沟通情况。
参与研究的胃肠病学家(美国15名;欧洲8名)确定符合条件且有预约门诊的患者。患者(美国40名;欧洲28名;年龄≥18岁;经医生判定为中度至重度活动性溃疡性结肠炎约≥1年;前一年至少有1次病情发作;曾接受或正在接受5-氨基水杨酸类药物和/或皮质类固醇治疗)同意对其门诊进行录音。分别对胃肠病学家和患者进行随访访谈。使用社会语言学方法分析文字记录,以探讨生活质量(QoL)影响、治疗目标和对治疗的态度。
在欧洲和美国的研究中,患者在门诊期间不讨论溃疡性结肠炎对生活质量影响的情况较为普遍。在美国的研究中,40%的病例中患者和医生在生活质量影响方面达成了完全一致(患者和医生表述的影响相同)。胃肠病学家和患者之间的治疗目标存在差异:3%的美国患者将无炎症作为治疗目标,而胃肠病学家的这一比例为25%。这一目标在门诊期间并非总是传达给患者。与指南一致,医生通常认为生物治疗适用于对传统治疗无效的患者。然而,尽管生物治疗的假定疗效通常与患者所述的治疗目标一致,但许多患者认为生物治疗更适用于比他们病情更严重的疾病。
患者和医生在溃疡性结肠炎对生活质量的影响、治疗目标以及对先进治疗的需求方面的一致性较差。需要新的工具来弥补这一差距。