Ehrenreich Hannelore
Clinical Neuroscience, Max Planck Institute of Experimental Medicine, DFG Research Center for Nanoscale Microscopy and Molecular Physiology of the Brain (CNMPB) , Göttingen , Germany.
Front Immunol. 2017 Mar 1;8:181. doi: 10.3389/fimmu.2017.00181. eCollection 2017.
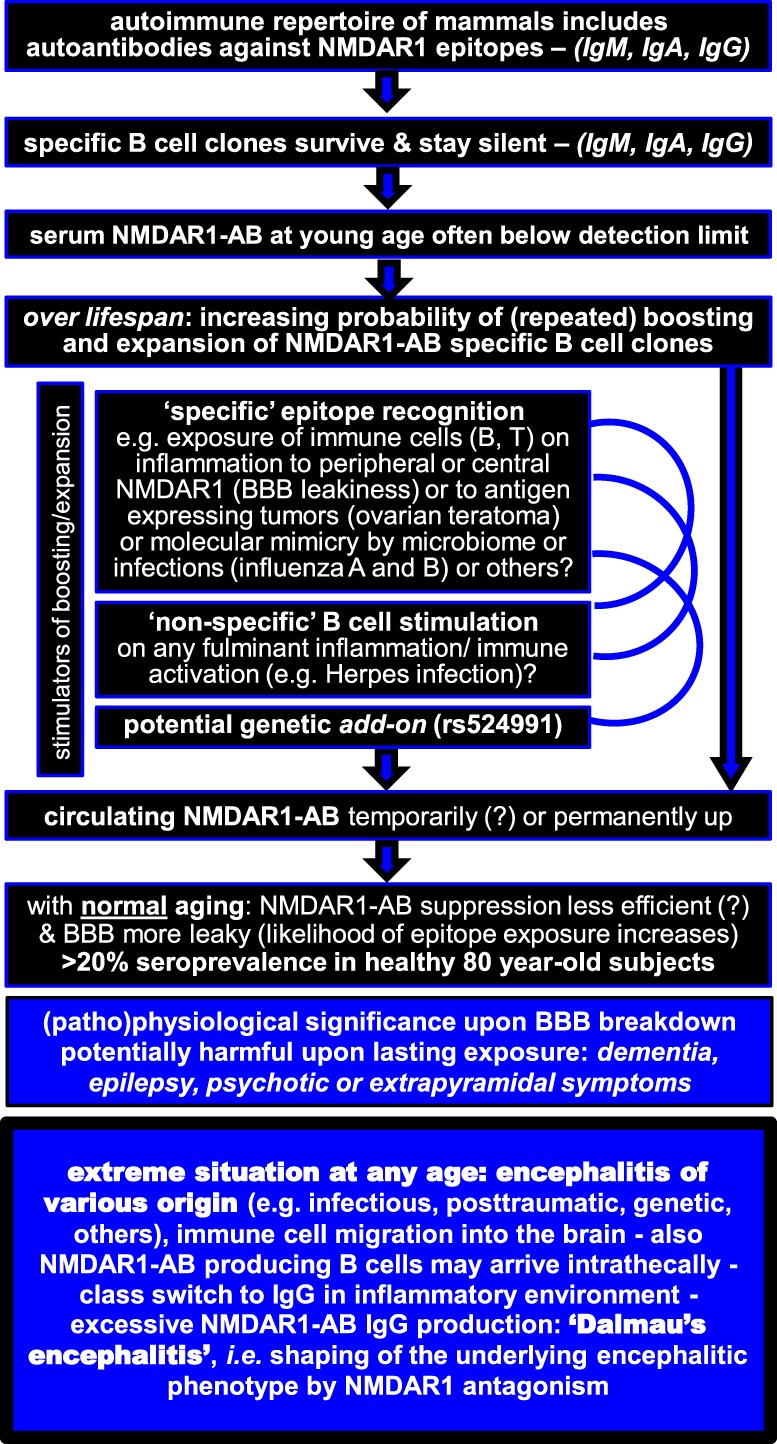
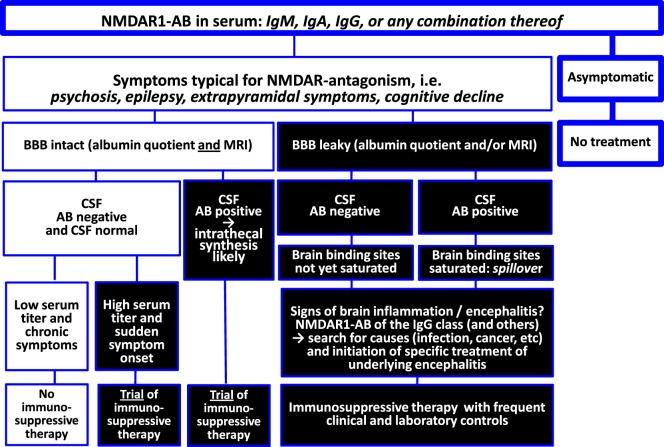
This viewpoint review provides an integrative picture of seemingly contradictory work published on -methyl-d-aspartate receptor 1 (NMDAR1) autoantibodies (AB). Based on the present state of knowledge, it gives recommendations for the clinical decision process regarding immunosuppressive treatment. Brain antigen-directed AB in general and NMDAR1-AB in particular belong to a preexisting autoimmune repertoire of mammals including humans. Specific autoimmune reactive B cells may get repeatedly (perhaps transiently) boosted by various potential stimulants (e.g., microbiome, infections, or neoplasms) plus less efficiently suppressed over lifespan (gradual loss of tolerance), likely explaining the increasing seroprevalence upon aging (>20% NMDAR1-AB in 80-year-old humans). Pathophysiological significance emerges (I) when AB-specific plasma cells settle in the brain and produce large amounts of brain antigen-directed AB intrathecally and/or (II) in conditions of compromised blood-brain barrier (BBB), for instance, upon injury, infection, inflammation, or genetic predisposition ( haplotype), which then allows substantial access of circulating AB to the brain. Regarding NMDAR1-AB, functional effects on neurons and elicitation of brain symptoms have been demonstrated for immunoglobulin (Ig) classes, IgM, IgA, and IgG. Under conditions of brain inflammation, intrathecal production and class switch to IgG may provoke high NMDAR1-AB (and other brain antigen-directed AB) levels in cerebrospinal fluid (CSF) and serum, causing the severe syndrome named "anti-NMDAR encephalitis," which then requires immunosuppressive therapy on top of the causal encephalitis treatment (if available). However, negative CSF NMDAR1-AB results cannot exclude chronic effects of serum NMDAR1-AB on the central nervous system, since the brain acts as "immunoprecipitator," particularly in situations of compromised BBB. In any case of suspected symptomatic consequences of circulating AB directed against brain antigens, leakiness of the BBB should be evaluated by CSF analysis (albumin quotient as proxy) and magnetic resonance imaging before considering immunosuppression.
这篇观点性综述对已发表的关于N-甲基-D-天冬氨酸受体1(NMDAR1)自身抗体(AB)的看似矛盾的研究进行了综合阐述。基于目前的知识水平,为免疫抑制治疗的临床决策过程提供了建议。一般而言,针对脑抗原的自身抗体,尤其是NMDAR1自身抗体,属于包括人类在内的哺乳动物预先存在的自身免疫库。特定的自身免疫反应性B细胞可能会被各种潜在刺激物(如微生物群、感染或肿瘤)反复(可能是短暂地)激活,并且在整个生命周期中抑制效率较低(耐受性逐渐丧失),这可能解释了随着年龄增长血清阳性率的增加(80岁人群中NMDAR1自身抗体阳性率>20%)。当AB特异性浆细胞定居在大脑中并在鞘内产生大量针对脑抗原的自身抗体时,以及/或者在血脑屏障(BBB)受损的情况下,例如受伤、感染、炎症或遗传易感性(单倍型)时,病理生理意义就会显现出来,此时循环中的自身抗体能够大量进入大脑。关于NMDAR1自身抗体,免疫球蛋白(Ig)类别IgM、IgA和IgG对神经元的功能影响以及脑症状的引发已经得到证实。在脑部炎症的情况下,鞘内产生并类别转换为IgG可能会导致脑脊液(CSF)和血清中NMDAR1自身抗体(以及其他针对脑抗原的自身抗体)水平升高,从而引发名为“抗NMDAR脑炎”的严重综合征,这就需要在病因性脑炎治疗(如果可行)的基础上进行免疫抑制治疗。然而,脑脊液NMDAR1自身抗体检测结果为阴性并不能排除血清NMDAR1自身抗体对中枢神经系统的慢性影响,因为大脑起到了“免疫沉淀器”的作用,尤其是在血脑屏障受损的情况下。在任何怀疑循环中针对脑抗原的自身抗体有症状性后果的情况下,在考虑免疫抑制之前,应通过脑脊液分析(以白蛋白商数作为指标)和磁共振成像评估血脑屏障的通透性。