Solazzo Antonio, Lassandro Giulia, Lassandro Francesco
Antonio Solazzo, Department of Radiology, AO Bolognini di Seriate, 24068 Seriate, Italy.
World J Radiol. 2017 Feb 28;9(2):85-90. doi: 10.4329/wjr.v9.i2.85.
To produce a radiological grading of gastric traumatic injuries.
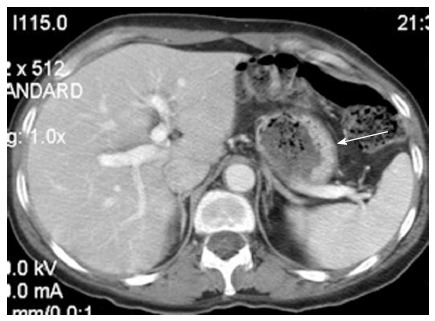
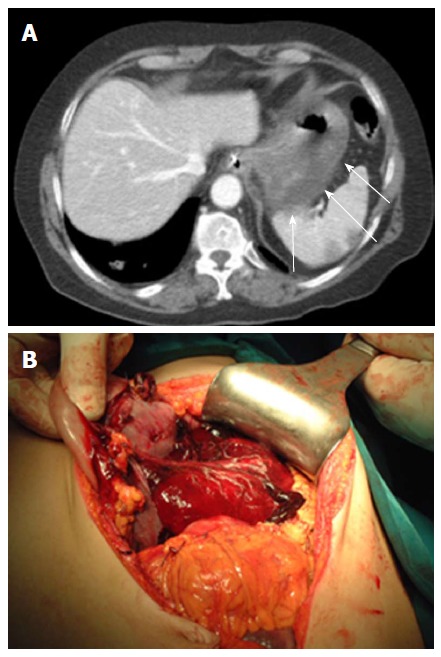
In our study, we retrospectively analyzed 32 cases of blunt gastric traumatic injuries and compared computed tomography (CT) data with patients' surgical or medical development. In all cases, a basal phase was acquired, and an intravenous contrast material was administered an antecubital venous catheter with acquisition in the venous phase (70-90 s). In addition, a further set of delayed scans was performed 4-5 min after the first scanning session, without supplementary intravenous contrast material, to identify or better define areas of active bleeding. All CT examinations were retrospectively reviewed by two radiologists, with more than 5 years of experience in emergency radiology, to detect signs of gastric injuries and/or associated abdominal lesions according to literature data. Specific CT findings for gastric rupture include luminal content extravasation and discontinuity of the gastric wall, while CT findings suggestive of injury consisted of free peritoneal fluid, extraluminal air, pneumatosis, and thickening and hematoma of gastric wall.
We found 32 gastric traumatic injuries. In 22 patients (68.8%), the diagnosis was based on the surgical findings; in the other 10 patients (31.2%), the diagnosis was based on the clinical and CT radiological data. We observed discontinuity of the gastric wall and luminal content extravasation in 1 patient (3.1%); in 10 patients (31.2%), there was extra-luminal air in the peritoneum. In 28 patients (87.5%), there was peritoneal fluid, which was blood in 14 patients (hematoma in 11 patients and contrast material extravasation from active bleeding in 3 patients). In 15 patients (46.9%), there was gastric wall thickening. In 3 patients, it was possible to identify a prevalent involvement of the external layer of the gastric wall, whereas, in 2 patients, the inner side of the gastric wall presented with major involvement. In 3 patients (9.4%), pneumatosis of the gastric wall was detected. In 19 (59.4%) patients, the stomach was full. The fundus was the most frequently damaged part of the stomach because it was involved in 17 patients (53.1%). Based on the observed data, we identified four grades of gastric lesions.
A radiologic score is helpful for guiding the diagnosis and management (surgical or conservative) of gastric blunt traumatic injuries and stratify patients according to short-term outcomes.
制定胃创伤性损伤的放射学分级。
在本研究中,我们回顾性分析了32例钝性胃创伤性损伤病例,并将计算机断层扫描(CT)数据与患者的手术或病情发展情况进行比较。所有病例均采集了基础期图像,并通过肘前静脉导管注入静脉造影剂,在静脉期(70 - 90秒)进行采集。此外,在首次扫描后4 - 5分钟进行另一组延迟扫描,不补充静脉造影剂,以识别或更好地界定活动性出血区域。两位具有超过5年急诊放射学经验的放射科医生对所有CT检查进行了回顾性分析,以根据文献数据检测胃损伤和/或相关腹部病变的迹象。胃破裂的特定CT表现包括腔内内容物外渗和胃壁连续性中断,而提示损伤的CT表现包括腹腔游离液体、腔外气体、积气以及胃壁增厚和血肿。
我们发现了32例胃创伤性损伤。22例患者(68.8%)的诊断基于手术结果;另外10例患者(31.2%)的诊断基于临床和CT放射学数据。我们观察到1例患者(3.1%)胃壁连续性中断和腔内内容物外渗;10例患者(31.2%)腹腔内有腔外气体。28例患者(87.5%)有腹腔积液,其中14例为血性积液(11例为血肿,3例为活动性出血导致的造影剂外渗)。15例患者(46.9%)胃壁增厚。3例患者中可确定胃壁外层受累为主,而2例患者胃壁内侧受累为主。3例患者(9.4%)检测到胃壁积气。19例(59.4%)患者胃呈充盈状态。胃底是最常受损的胃部位,17例患者(53.1%)受累。根据观察到的数据,我们确定了四级胃损伤。
放射学评分有助于指导胃钝性创伤性损伤的诊断和处理(手术或保守治疗),并根据短期预后对患者进行分层。