Jochmans Ina, Monbaliu Diethard, Ceulemans Laurens J, Pirenne Jacques, Fronek Jiri
Abdominal Transplant Surgery, University Hospitals Leuven, Leuven, Belgium.
Department of Microbiology and Immunology, Lab of Abdominal Transplant Surgery, KU Leuven, Leuven, Belgium.
PLoS One. 2017 Mar 17;12(3):e0174123. doi: 10.1371/journal.pone.0174123. eCollection 2017.
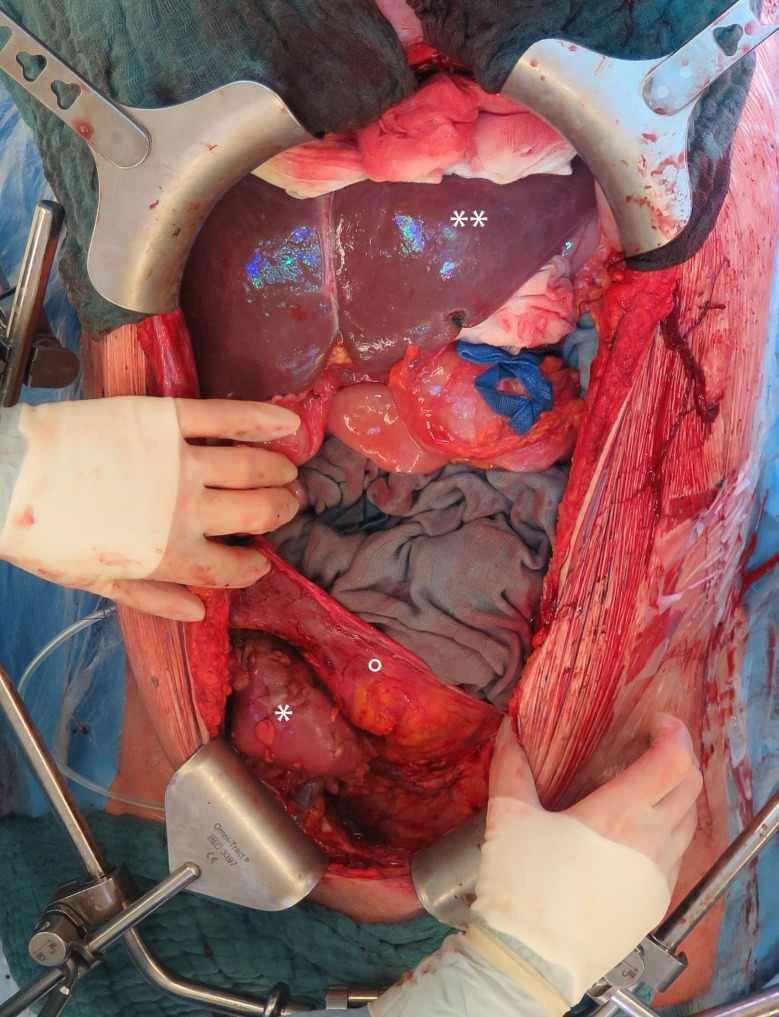
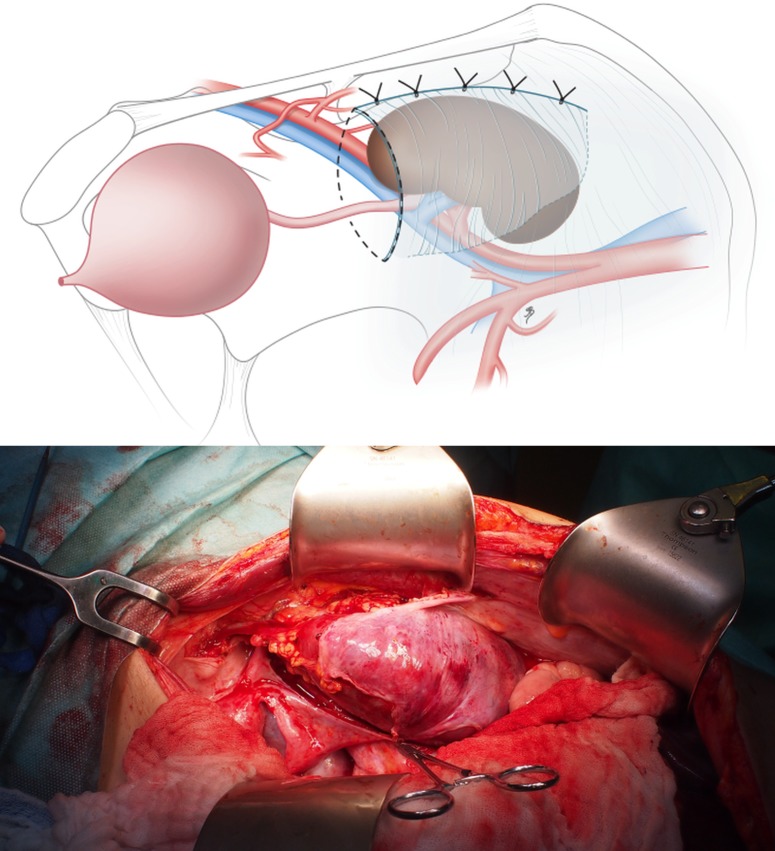
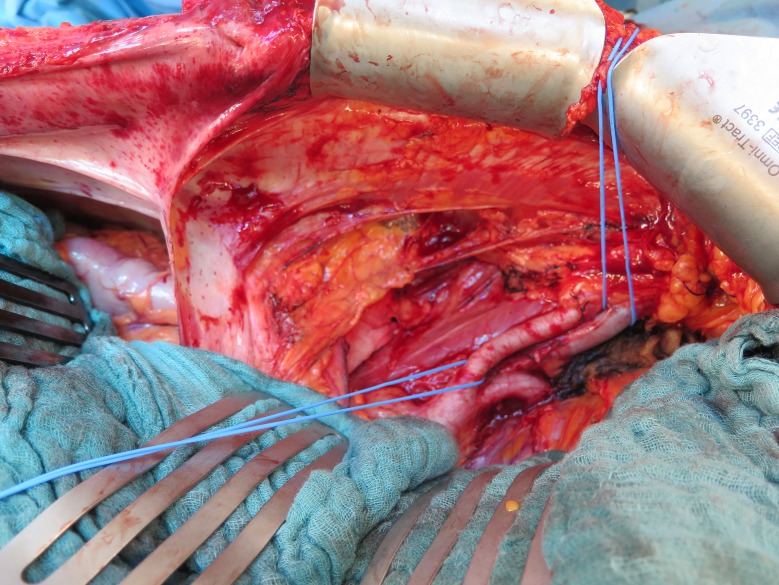
In Eurotransplant, 50% of simultaneous liver kidney transplantations (SLK) are performed for polycystic disease. Classically, liver and kidney are transplanted in two steps: liver through a subcostal incision, kidney through a separate oblique incision. Liver and kidney volume can make this 'two-step' procedure challenging, especially if simultaneous native nephrectomy is indicated. A 'one-step' SLK through a xiphopubic laparotomy might be a safe alternative, facilitating mobilization of the voluminous polycystic liver and native nephrectomy whilst offering access to iliac fossae for kidney transplantation. One-step SLK procedures for polycystic disease were introduced in 08/2013 at IKEM Prague (n = 6) and 11/2014 at University Hospitals Leuven (n = 6). Feasibility and safety of the one-step technique were investigated. We compared surgical data and outcomes obtained with the one-step technique to all consecutive two-step procedures performed for polycystic disease at the University Hospitals Leuven between 2008-2014 (n = 23). Median (interquartile range) are given. One-step SLK offered broad and adequate exposure for the hepatectomy, nephrectomies and transplantations, which were all uneventful. Morbidity, patient (100% vs 91%, p = 0.53) and graft survival (100% graft survival for liver and kidney in both groups) were comparable between one-step and two-step SLK. Liver cold ischaemia time was comparable [6.0 (4.4-7.6) vs. 7.1 (3.9-7.3), p = 0.077], kidney cold ischaemia time was shorter in one-step compared to two-step SLK [8.1 (6.4-9.3) vs. 11.7 (10.0-14.0), p<0.001)]. Total procedural time was also shorter in one-step compared to two-step SLK [6.8 (4.1-9.3) vs. 9.0 (8.7-10.1), p = 0.032], while all underwent bilateral (67%) or unilateral (33%) nephrectomy (compared to 0% and 52% in two-step SLK, respectively). In one-step SLK, 67% received a pre-emptive kidney transplant compared to 46% in two-step SLK. 5/12 two-step SLK became dialysis dependant after pre-transplant nephrectomy, the 4 dialysis-dependant patients with one-step SLK had not undergone pre-transplant nephrectomy. In conclusion, one-step SLK for polycystic disease is feasible and safe.
在欧洲器官移植组织中,50%的肝肾联合移植(SLK)是针对多囊肾病进行的。传统上,肝脏和肾脏分两步移植:肝脏通过肋下切口,肾脏通过单独的斜切口。肝脏和肾脏的体积可能使这种“两步”手术具有挑战性,特别是在需要同时切除自体肾的情况下。通过剑突耻骨上剖腹术进行的“一步”SLK可能是一种安全的替代方法,便于移动体积较大的多囊肝和切除自体肾,同时为肾脏移植提供进入髂窝的途径。针对多囊肾病的一步SLK手术于2013年8月在布拉格IKEM医院(n = 6)以及2014年11月在鲁汶大学医院(n = 6)开始实施。对一步技术的可行性和安全性进行了研究。我们将一步技术获得的手术数据和结果与2008 - 2014年期间在鲁汶大学医院针对多囊肾病进行的所有连续两步手术(n = 23)进行了比较。给出了中位数(四分位间距)。一步SLK为肝切除术、肾切除术和移植术提供了广泛且充分的暴露,所有手术均顺利进行。一步和两步SLK在发病率、患者生存率(100%对91%,p = 0.53)和移植物生存率(两组肝脏和肾脏移植物生存率均为100%)方面具有可比性。肝脏冷缺血时间具有可比性[6.0(4.4 - 7.6)对7.1(3.9 - 7.3),p = 0.077],与两步SLK相比,一步SLK的肾脏冷缺血时间更短[8.1(6.4 - 9.3)对11.7(10.0 - 14.0),p<0.001]。与两步SLK相比,一步SLK的总手术时间也更短[6.8(4.1 - 9.3)对9.0(8.7 - 10.1),p = 0.032],同时所有患者均接受了双侧(67%)或单侧(33%)肾切除术(相比之下,两步SLK分别为0%和52%)。在一步SLK中,67%的患者接受了预防性肾脏移植,而两步SLK中这一比例为46%。5/12例两步SLK在移植前肾切除术后需要依赖透析,而4例依赖透析的一步SLK患者未进行移植前肾切除术。总之,针对多囊肾病的一步SLK是可行且安全的。