Kwatra Vineet, Karanth Narayan V, Priyadarshana Kelum, Charakidis Michail
Medical Oncology Department, Alan Walker Cancer Centre, Royal Darwin Hospital, 105 Rocklands Drive, Tiwi, NT, 0810, Australia.
NT Renal Services, Royal Darwin Hospital, Darwin, NT, Australia.
J Med Case Rep. 2017 Mar 19;11(1):73. doi: 10.1186/s13256-017-1229-z.
Transplant patients were excluded from the pivotal phase III trials of checkpoint inhibitors in metastatic melanoma. The efficacy and toxicity profiles of checkpoint inhibitors in this cohort of patients are not well described. To the best of our knowledge, this is the first case report of a renal transplant patient with stage IV melanoma treated with a programmed cell death protein 1 checkpoint inhibitor that led to both treatment failure and renal graft rejection.
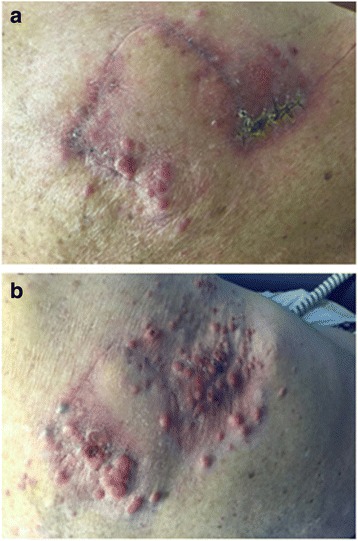
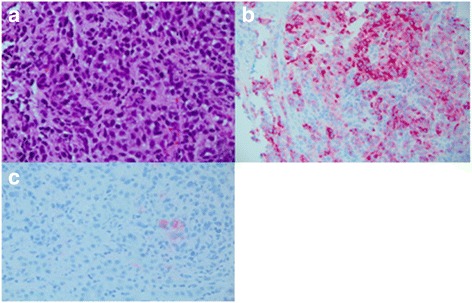
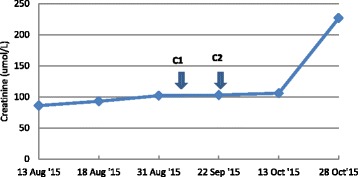
We present a case of a 58-year-old white man with a long-standing cadaveric renal transplant who was diagnosed with a B-Raf Proto-Oncogene, Serine/Threonine Kinase wild-type metastatic melanoma. He was treated with first-line pembrolizumab but experienced subsequent graft failure and rapid disease progression.
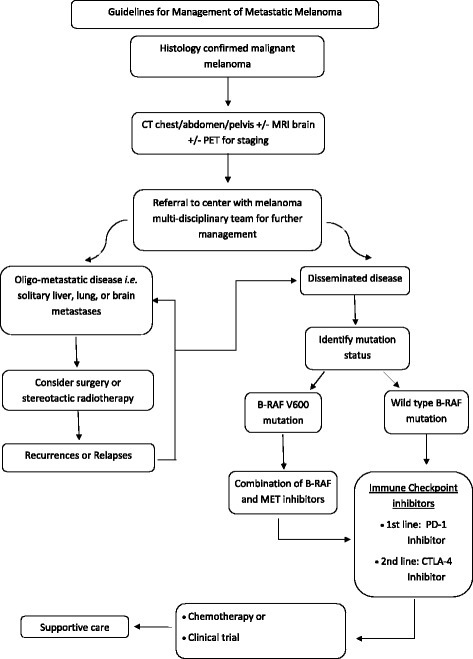
This case highlights the risks associated with the administration of checkpoint inhibitors in patients with a renal transplant and on immunosuppressive therapy. More specifically, it adds to the literature indicating that, compared with the cytotoxic T-lymphocyte-associated protein 4 inhibitor ipilimumab, anti-programmed cell death protein 1 agents are more likely to lead to renal graft failure. Additionally, these novel immunotherapeutics may be ineffective in transplant patients; therefore, clinicians should be very aware of those risks and carefully consider selection of agents and full disclosure of the risks to their patients.
在转移性黑色素瘤的关键III期试验中,移植患者被排除在外。检查点抑制剂在这类患者中的疗效和毒性特征尚未得到充分描述。据我们所知,这是首例肾移植患者接受程序性细胞死亡蛋白1检查点抑制剂治疗IV期黑色素瘤导致治疗失败和肾移植排斥的病例报告。
我们报告一例58岁白人男性,长期接受尸体肾移植,被诊断为B-Raf原癌基因丝氨酸/苏氨酸激酶野生型转移性黑色素瘤。他接受了一线派姆单抗治疗,但随后出现移植失败和疾病快速进展。
该病例突出了肾移植且接受免疫抑制治疗的患者使用检查点抑制剂相关的风险。更具体地说,这一病例补充了文献内容,表明与细胞毒性T淋巴细胞相关蛋白4抑制剂伊匹单抗相比,抗程序性细胞死亡蛋白1药物更易导致肾移植失败。此外,这些新型免疫疗法在移植患者中可能无效;因此,临床医生应充分认识到这些风险,并仔细考虑药物选择以及向患者充分披露风险。