Chen Jiao, Clark Leslie H, Kong Wei-Min, Yan Zhen, Han Chao, Zhao Hui, Liu Ting-Ting, Zhang Tong-Qing, Song Dan, Jiao Si-Meng, Zhou Chunxiao
Department of Gynecological Oncology, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing, China.
Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, United States of America.
PLoS One. 2017 Mar 23;12(3):e0174226. doi: 10.1371/journal.pone.0174226. eCollection 2017.
Prior studies evaluating the impact of hysteroscopy on outcomes in endometrial cancer have predominantly evaluated type I tumors. We sought to evaluate whether hysteroscopy worsens prognosis in type II endometrial cancer.
A retrospective cohort analysis of 140 patients from two institutions with type II endometrial cancer was performed. Women who underwent either diagnostic hysteroscopy (HSC) or dilation and curettage (D&C) for cancer diagnosis from June 2001 until June 2010 were included. The clinical and pathologic characteristics, including peritoneal cytology results were reviewed. The primary endpoint was disease-specific survival (DSS). The exposure of interest was hysteroscopy. Survival curves were projected using the Kaplan-Meier method and compared using the log-rank test.
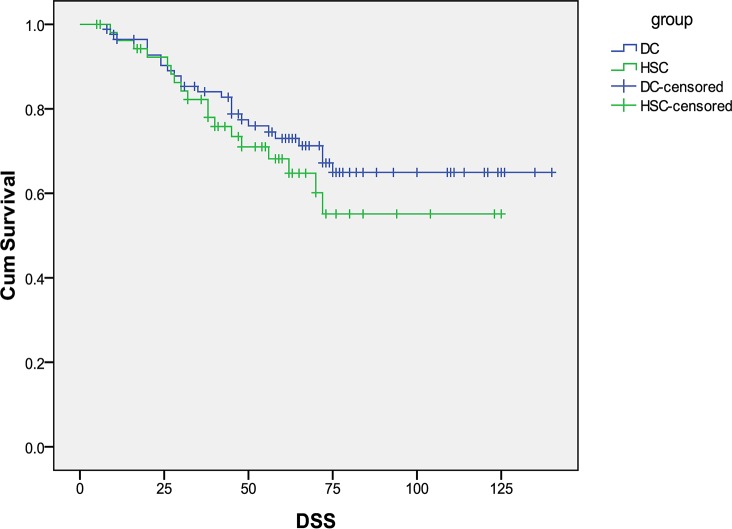
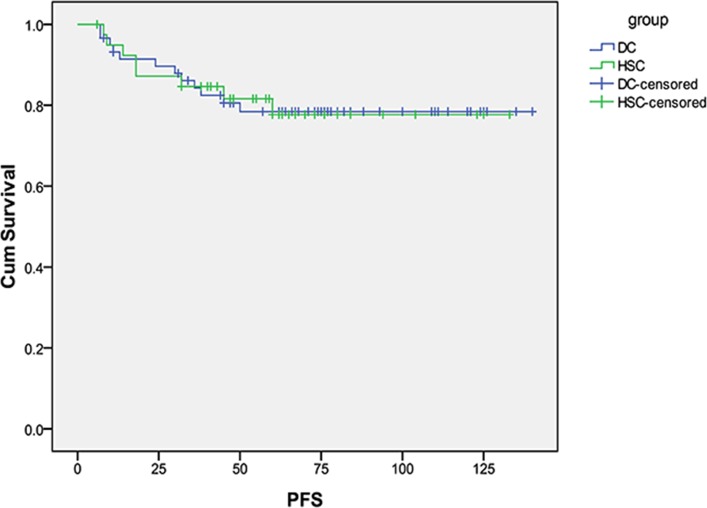
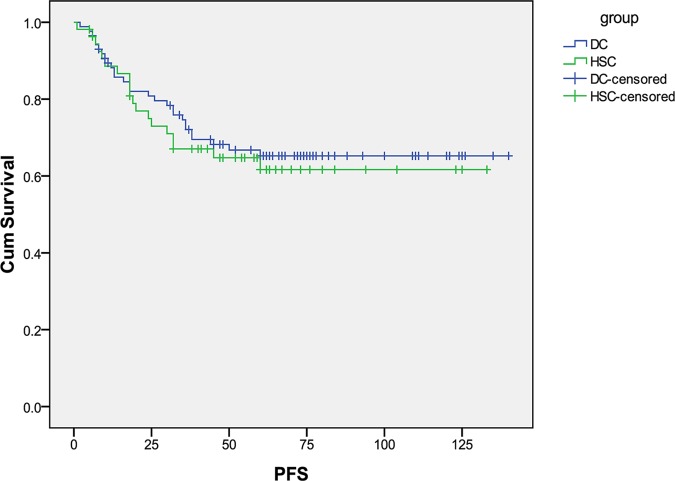
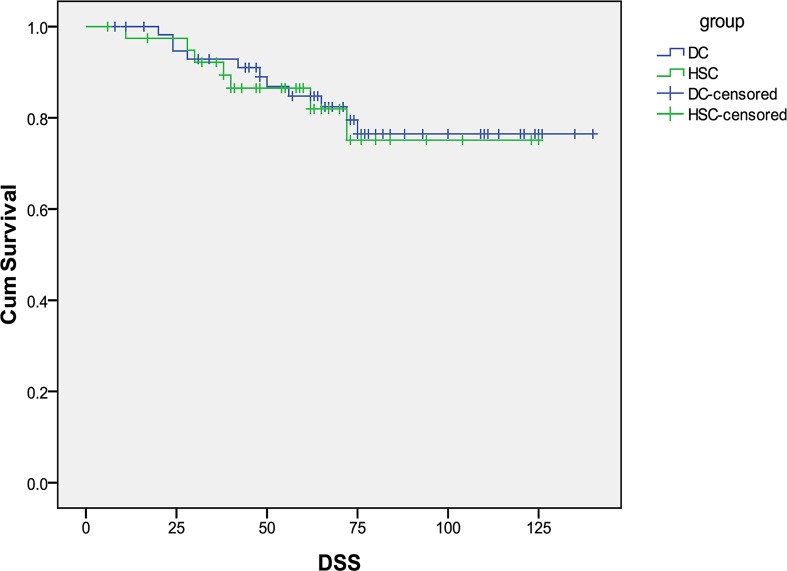
There was no difference in age, histology, stage, depth of myometrial invasion, adnexal involvement, or nodal metastasis between HSC and D&C patients. Positive cytology was found in 16/54 (30%) patients following HSC and in 10/86 (12%) following D&C (p = 0.008). Fourteen patients with stage I and II disease had positive peritoneal cytology, with 11/40 (27.5%) patients in the HSC group and 3/59 (5%) patients in the D&C group(p = 0.002). Median DSS was clinically different for the HSC and D&C groups, but statistical significance was not reached (53 versus 63.5 months, p = 0.34). For stage I and II patients, 18/99 (18%) were dead of EC, with a median DSS of 60 months for HSC and 71 months for D&C (p = 0.82). Overall 46 (33%) patients developed a recurrence, with 18/54 (33%) in the HSC group compared to 28/86 (32%) in the D&C group (p = 0.92). There was no difference in recurrence location between groups.
Diagnostic hysteroscopy significantly increased the rate of positive peritoneal cytology at the time of surgical staging in this cohort of patients with type II EC. However, we were unable to detect a difference in prognosis as measured by DSS.
先前评估宫腔镜检查对子宫内膜癌预后影响的研究主要针对I型肿瘤。我们旨在评估宫腔镜检查是否会使II型子宫内膜癌的预后恶化。
对来自两家机构的140例II型子宫内膜癌患者进行回顾性队列分析。纳入2001年6月至2010年6月期间因癌症诊断而接受诊断性宫腔镜检查(HSC)或刮宫术(D&C)的女性。回顾了临床和病理特征,包括腹腔细胞学检查结果。主要终点是疾病特异性生存率(DSS)。感兴趣的暴露因素是宫腔镜检查。使用Kaplan-Meier方法绘制生存曲线,并使用对数秩检验进行比较。
HSC组和D&C组在年龄、组织学、分期、肌层浸润深度、附件受累或淋巴结转移方面无差异。HSC术后16/54(30%)患者腹腔细胞学检查阳性,D&C术后10/86(12%)患者阳性(p = 0.008)。14例I期和II期疾病患者腹腔细胞学检查阳性,HSC组11/40(27.5%),D&C组3/59(5%)(p = 0.002)。HSC组和D&C组的中位DSS在临床上有差异,但未达到统计学意义(53个月对63.5个月,p = 0.34)。对于I期和II期患者,18/99(18%)死于子宫内膜癌,HSC组的中位DSS为60个月,D&C组为71个月(p = 0.82)。总体而言,46例(33%)患者出现复发,HSC组18/54(33%),D&C组28/86(32%)(p = 0.92)。两组之间的复发部位无差异。
在这组II型子宫内膜癌患者中,诊断性宫腔镜检查显著增加了手术分期时腹腔细胞学检查阳性的发生率。然而,我们未能检测到以DSS衡量的预后差异。