Thornton Hannah V, Hay Alastair D, Redmond Niamh M, Turnbull Sophie L, Christensen Hannah, Peters Tim J, Leeming John P, Lovering Andrew, Vipond Barry, Muir Peter, Blair Peter S
Centre for Academic Primary Care, School of Social and Community Medicine, University of Bristol, Bristol, UK.
National Institute for Health Research Collaborations for Leadership in Applied Health Research and Care West (NIHR CLAHRC West), University Hospitals Bristol NHS Foundation Trust, Bristol, UK.
Fam Pract. 2017 Aug 1;34(4):407-415. doi: 10.1093/fampra/cmw136.
Diagnostic uncertainty over respiratory tract infections (RTIs) in primary care contributes to over-prescribing of antibiotics and drives antibiotic resistance. If symptoms and signs predict respiratory tract microbiology, they could help clinicians target antibiotics to bacterial infection. This study aimed to determine relationships between symptoms and signs in children presenting to primary care and microbes from throat swabs.
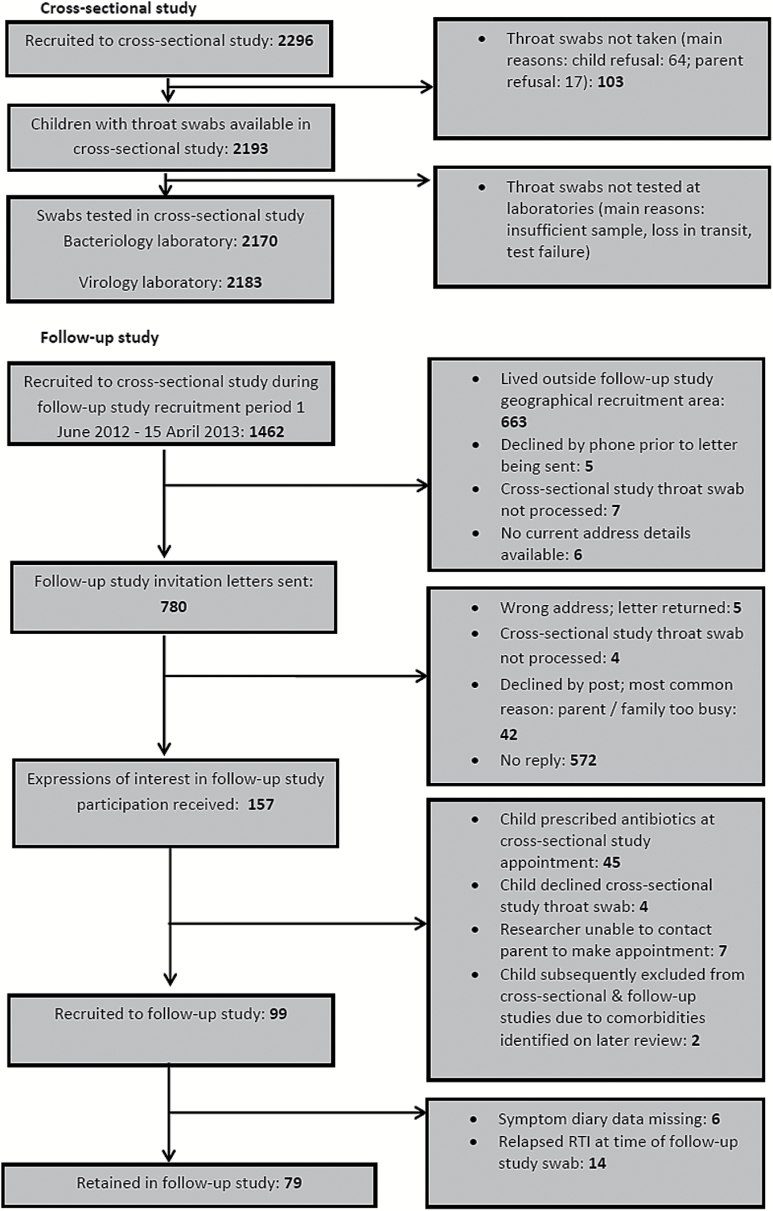
Cross-sectional study of children ≥3 months to <16 years presenting with acute cough and RTI, with subset follow-up. Associations and area under receiver operating curve (AUROC) statistics sought between clinical presentation and baseline microbe detection. Microbe prevalence compared between baseline (symptomatic) and follow-up (asymptomatic) visits.
At baseline, ≥1 bacteria was detected in 1257/2113 (59.5%) children and ≥1 virus in 894/2127 (42%) children. Clinical presentation was not associated with detection of ≥1 bacteria [AUROC 0.54 (95% CI 0.52-0.56)] or ≥1 virus [0.64 (95% CI 0.61-0.66)]. Individually, only respiratory syncytial virus (RSV) was associated with clinical presentation [AUROC 0.80 (0.77-0.84)]. Prevalence fell between baseline and follow-up; more so in viruses (68% versus 26%, P < 0.001) than bacteria (56% versus 40%, P = 0.01); greatest reductions seen in RSV, influenza B and Haemophilus influenzae.
Findings demonstrate that clinical presentation cannot distinguish the presence of bacteria or viruses in the upper respiratory tract. However, individual and overall microbe prevalence was greater when children were unwell than when well, providing some evidence that upper respiratory tract microbes may be the cause or consequence of the illness. If causal, selective microbial point-of-care testing could be beneficial.
基层医疗中呼吸道感染(RTIs)的诊断不确定性导致抗生素过度处方,并推动了抗生素耐药性。如果症状和体征能够预测呼吸道微生物情况,它们可以帮助临床医生将抗生素应用于细菌感染。本研究旨在确定基层医疗中就诊儿童的症状和体征与咽拭子微生物之间的关系。
对年龄≥3个月至<16岁出现急性咳嗽和呼吸道感染的儿童进行横断面研究,并进行亚组随访。在临床表现与基线微生物检测之间寻求关联及受试者工作特征曲线下面积(AUROC)统计。比较基线(有症状)和随访(无症状)就诊时的微生物患病率。
在基线时,2113名儿童中有1257名(59.5%)检测到≥1种细菌,2127名儿童中有894名(42%)检测到≥1种病毒。临床表现与检测到≥1种细菌[AUROC 0.54(95%CI 0.52 - 0.56)]或≥1种病毒[0.64(95%CI 0.61 - 0.66)]无关。单独来看,只有呼吸道合胞病毒(RSV)与临床表现相关[AUROC 0.80(0.77 - 0.84)]。患病率在基线和随访之间下降;病毒下降幅度更大(68%对26%,P < 0.001),细菌下降幅度较小(56%对40%,P = 0.01);呼吸道合胞病毒、乙型流感病毒和流感嗜血杆菌下降幅度最大。
研究结果表明,临床表现无法区分上呼吸道中细菌或病毒的存在。然而,儿童不适时个体及总体微生物患病率高于健康时,这提供了一些证据表明上呼吸道微生物可能是疾病的原因或结果。如果是因果关系,选择性微生物即时检测可能有益。