Krych Michalina, Biernacka Elżbieta Katarzyna, Ponińska Joanna, Kukla Piotr, Filipecki Artur, Gajda Robert, Hasdemir Can, Antzelevitch Charles, Kosiec Agnieszka, Szperl Małgorzata, Płoski Rafał, Trusz-Gluza Maria, Mizia-Stec Katarzyna, Hoffman Piotr
Department of Congenital Cardiac Defects, Institute of Cardiology, Warsaw, Poland.
Department of Congenital Cardiac Defects, Institute of Cardiology, Warsaw, Poland.
J Cardiol. 2017 Nov;70(5):504-510. doi: 10.1016/j.jjcc.2017.01.009. Epub 2017 Mar 21.
Andersen-Tawil syndrome (ATS) is rare channelopathy caused by KCNJ2 mutation and probably KCNJ5. It is characterized by arrhythmias, neurological symptoms, and dysmorphic features. The present study retrospectively examined the characteristics of 11 unrelated families with ATS.
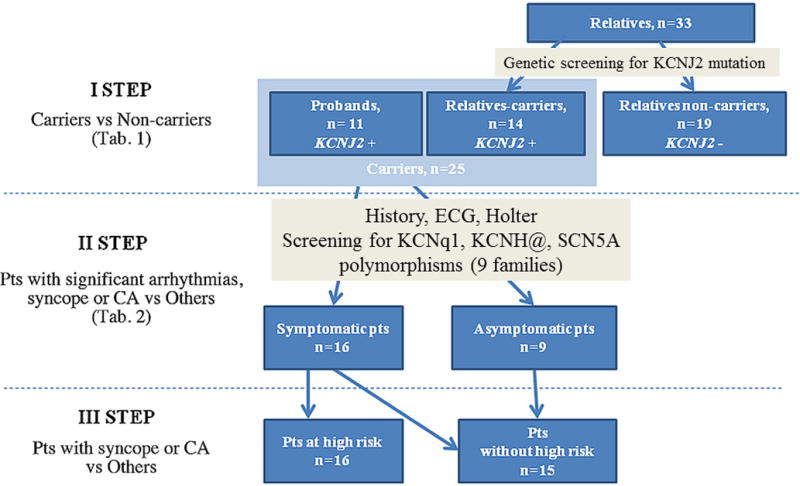
This study consisted of 11 probands positive for KCNJ2 variants and 33 family members (mean age 30.0±17.3 years, female n=31). Additional genetic screening of 3 LQTS genes (KCNQ1, KCNH2, SCN5A) was performed in 9 families. Predictors of arrhythmias [premature ventricular beats>2000/24h, biventricular and polymorphic ventricular tachycardia (VT)], syncope, and/or cardiac arrest (CA) were evaluated.
In KCNJ2 mutation carriers vs non-carriers (n=25 vs n=19) significant differences were observed in U-wave manifestations in V2-V4, T-T duration, QTUc duration (p<0.0001), dysmorphic features, and neurological symptoms. Compared to asymptomatic carriers (n=9), in those with arrhythmias and/or syncope and/or CA (n=16) micrognathia (p=0.004), periodic paralysis (p=0.019), palpitation (p=0.005), U-wave n V2-V4 (p=0.049) were more frequent; QTU (p=0.045) and T-T (p=0.014) were also longer (n=9). In the subgroup of carriers with syncope and/or cardiac arrest (n=10, 90% women), K897T-KCNH2 polymorphism (p=0.02), periodic paralysis (p=0.004), muscle weakness (p=0.04), palpitations (p=0.04), arrhythmias (biventricular VT, p=0.003; polymorphic VT, p=0.009) were observed more frequently. T-T duration was longer (p=0.007) and the percentage of patients with premature ventricular contraction >2000/24h was higher (p=0.005).
A higher risk of arrhythmia, syncope, and/or CA is associated with the presence of micrognathia, periodic paralysis, and prolonged T-T time. Our findings suggest that K897T may contribute to the occurrence of syncope.
安德森-塔维尔综合征(ATS)是一种由KCNJ2突变以及可能的KCNJ5突变引起的罕见通道病。其特征为心律失常、神经症状和畸形特征。本研究回顾性分析了11个无关的ATS家族的特征。
本研究包括11名KCNJ2变异阳性的先证者和33名家庭成员(平均年龄30.0±17.3岁,女性31名)。对9个家族进行了3种长QT综合征基因(KCNQ1、KCNH2、SCN5A)的额外基因筛查。评估心律失常[室性早搏>2000/24小时、双心室和多形性室性心动过速(VT)]、晕厥和/或心脏骤停(CA)的预测因素。
在KCNJ2突变携带者与非携带者(分别为25名和19名)中,观察到V2-V4导联U波表现、T-T间期、QTUc间期(p<0.0001)、畸形特征和神经症状存在显著差异。与无症状携带者(9名)相比,有心律失常和/或晕厥和/或CA的患者(16名)小颌畸形(p=0.004)、周期性瘫痪(p=0.019)、心悸(p=0.005)、V2-V4导联U波(p=0.049)更为常见;QTU(p=0.045)和T-T(p=0.014)也更长(9名)。在晕厥和/或心脏骤停的携带者亚组中(10名,90%为女性),K897T-KCNH2多态性(p=0.02)、周期性瘫痪(p=0.004)、肌肉无力(p=0.04)、心悸(p=0.04)、心律失常(双心室VT,p=0.003;多形性VT,p=0.009)更为常见。T-T间期更长(p=0.007),室性早搏>2000/24小时的患者百分比更高(p=0.005)。
小颌畸形、周期性瘫痪和T-T时间延长与心律失常、晕厥和/或CA的较高风险相关。我们的研究结果表明,K897T可能导致晕厥的发生。