Cavero Teresa, Rabasco Cristina, López Antía, Román Elena, Ávila Ana, Sevillano Ángel, Huerta Ana, Rojas-Rivera Jorge, Fuentes Carolina, Blasco Miquel, Jarque Ana, García Alba, Mendizabal Santiago, Gavela Eva, Macía Manuel, Quintana Luis F, María Romera Ana, Borrego Josefa, Arjona Emi, Espinosa Mario, Portolés José, Gracia-Iguacel Carolina, González-Parra Emilio, Aljama Pedro, Morales Enrique, Cao Mercedes, Rodríguez de Córdoba Santiago, Praga Manuel
Department of Nephrology, Instituto de Investigación Hospital 12 de Octubre (imas12), Madrid, Spain.
Department of Nephrology, University Hospital Reina Sofía, Córdoba, Spain.
Nephrol Dial Transplant. 2017 Mar 1;32(3):466-474. doi: 10.1093/ndt/gfw453.
Complement dysregulation occurs in thrombotic microangiopathies (TMAs) other than primary atypical haemolytic uraemic syndrome (aHUS). A few of these patients have been reported previously to be successfully treated with eculizumab.
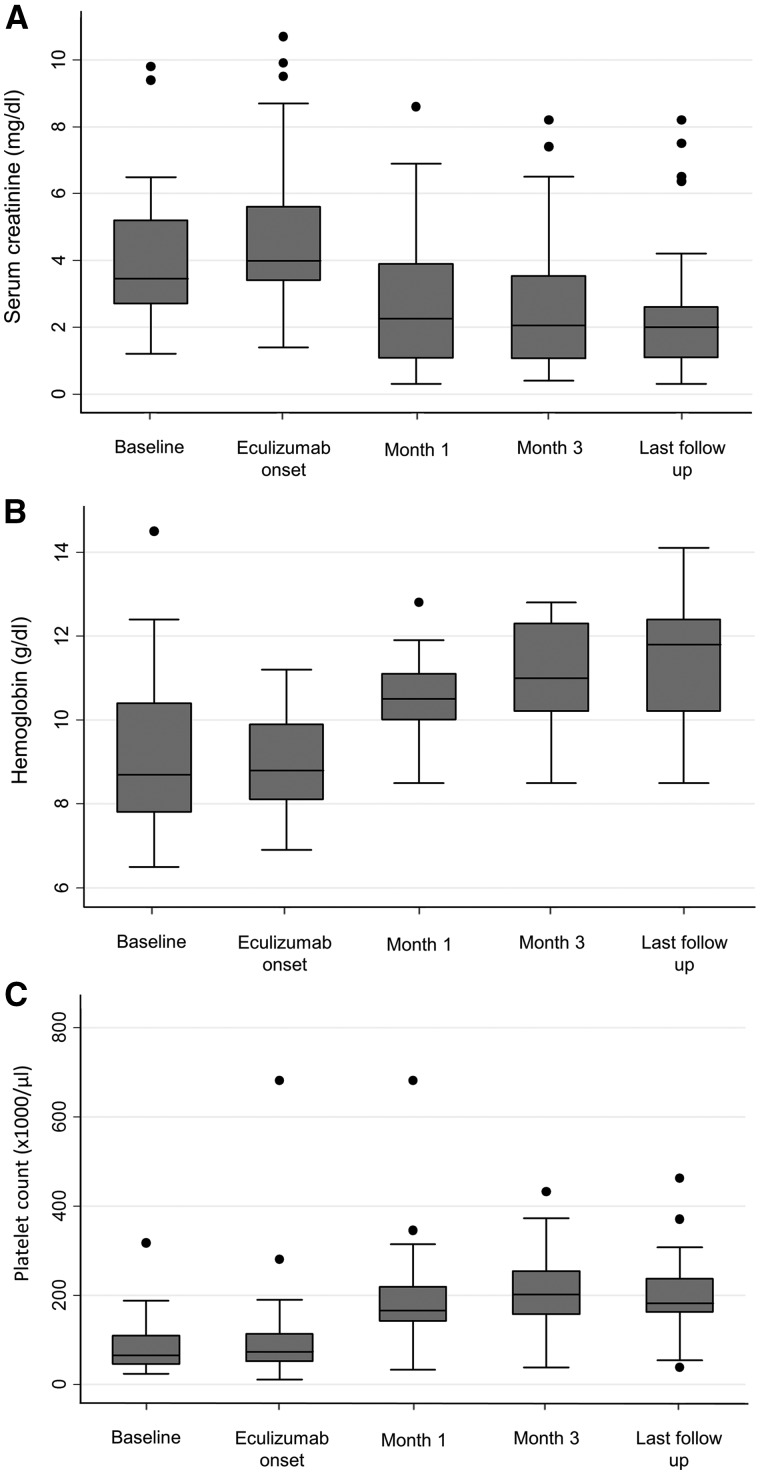
We identified 29 patients with so-called secondary aHUS who had received eculizumab at 11 Spanish nephrology centres. Primary outcome was TMA resolution, defined by a normalization of platelet count (>150 × 10 9 /L) and haemoglobin, disappearance of all the markers of microangiopathic haemolytic anaemia (MAHA), and improvement of renal function, with a ≥25% reduction of serum creatinine from the onset of eculizumab administration.
Twenty-nine patients with secondary aHUS (15 drug-induced, 8 associated with systemic diseases, 2 with postpartum, 2 with cancer-related, 1 associated with acute humoral rejection and 1 with intestinal lymphangiectasia) were included in this study. The reason to initiate eculizumab treatment was worsening of renal function and persistence of TMA despite treatment of the TMA cause and plasmapheresis. All patients showed severe MAHA and renal function impairment (14 requiring dialysis) prior to eculizumab treatment and 11 presented severe extrarenal manifestations. A rapid resolution of the TMA was observed in 20 patients (68%), 15 of them showing a ≥50% serum creatinine reduction at the last follow-up. Comprehensive genetic and molecular studies in 22 patients identified complement pathogenic variants in only 2 patients. With these two exceptions, eculizumab was discontinued, after a median of 8 weeks of treatment, without the occurrence of aHUS relapses.
Short treatment with eculizumab can result in a rapid improvement of patients with secondary aHUS in whom TMA has persisted and renal function worsened despite treatment of the TMA-inducing condition.
补体调节异常发生在除原发性非典型溶血尿毒综合征(aHUS)之外的血栓性微血管病(TMA)中。此前已有少数这类患者接受依库珠单抗治疗取得成功的报道。
我们在11家西班牙肾脏病中心确定了29例接受依库珠单抗治疗的所谓继发性aHUS患者。主要结局为TMA缓解,定义为血小板计数(>150×10⁹/L)和血红蛋白恢复正常,微血管病性溶血性贫血(MAHA)所有标志物消失,以及肾功能改善,即自依库珠单抗给药开始血清肌酐降低≥25%。
本研究纳入了29例继发性aHUS患者(15例药物性、8例与全身性疾病相关、2例产后、2例与癌症相关、1例与急性体液排斥相关、1例与肠淋巴管扩张相关)。开始依库珠单抗治疗的原因是尽管对TMA病因进行了治疗且进行了血浆置换,但肾功能仍恶化且TMA持续存在。所有患者在依库珠单抗治疗前均表现出严重的MAHA和肾功能损害(14例需要透析),11例有严重的肾外表现。20例患者(68%)观察到TMA迅速缓解,其中15例在最后一次随访时血清肌酐降低≥50%。对22例患者进行的全面基因和分子研究仅在2例患者中发现了补体致病变异。除这两例外,在中位治疗8周后停用依库珠单抗,未发生aHUS复发。
对于尽管对TMA诱发情况进行了治疗但TMA仍持续存在且肾功能恶化的继发性aHUS患者,短期使用依库珠单抗治疗可使其迅速改善。