Mathur Amit K, Chakrabarti Apurba K, Mellinger Jessica L, Volk Michael L, Day Ryan, Singer Andrew L, Hewitt Winston R, Reddy Kunam S, Moss Adyr A
Amit K Mathur, Ryan Day, Andrew L Singer, Winston R Hewitt, Kunam S Reddy, Adyr A Moss, Division of Transplant Surgery, Department of Surgery, Mayo Clinic Arizona, Phoenix, AZ 85054, United States.
World J Gastroenterol. 2017 Mar 14;23(10):1857-1865. doi: 10.3748/wjg.v23.i10.1857.
To determine whether hospital characteristics predict cirrhosis mortality and how much variation in mortality is attributable to hospital differences.
We used data from the 2005-2011 Nationwide Inpatient Sample and the American Hospital Association Annual survey to identify hospitalizations for decompensated cirrhosis and corresponding facility characteristics. We created hospital-specific risk and reliability-adjusted odds ratios for cirrhosis mortality, and evaluated patient and facility differences based on hospital performance quintiles. We used hierarchical regression models to determine the effect of these factors on mortality.
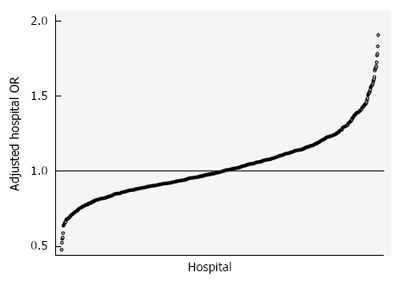
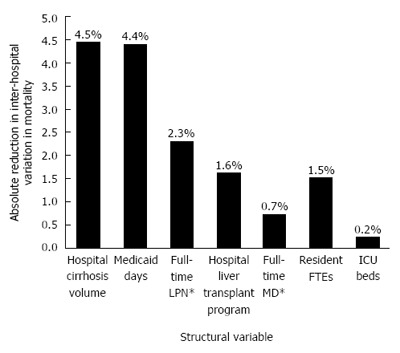
Seventy-two thousand seven hundred and thirty-three cirrhosis admissions were evaluated in 805 hospitals. Hospital mean cirrhosis annual case volume was 90.4 (range 25-828). Overall hospital cirrhosis mortality rate was 8.00%. Hospital-adjusted odds ratios (aOR) for mortality ranged from 0.48 to 1.89. Patient characteristics varied significantly by hospital aOR for mortality. Length of stay averaged 6.0 ± 1.6 days, and varied significantly by hospital performance ( < 0.001). Facility level predictors of risk-adjusted mortality were higher Medicaid case-mix (OR = 1.00, = 0.029) and LPN staffing (OR = 1.02, = 0.015). Higher cirrhosis volume (OR = 0.99, = 0.025) and liver transplant program status (OR = 0.83, = 0.026) were significantly associated with survival. After adjusting for patient differences, era, and clustering effects, 15.3% of variation between hospitals was attributable to differences in facility characteristics.
Hospital characteristics account for a significant proportion of variation in cirrhosis mortality. These findings have several implications for patients, providers, and health care delivery in liver disease care and inpatient health care design.
确定医院特征是否能预测肝硬化死亡率,以及死亡率的多少差异可归因于医院差异。
我们使用了2005 - 2011年全国住院患者样本数据和美国医院协会年度调查数据,以确定失代偿期肝硬化的住院情况及相应的医院特征。我们创建了针对医院的肝硬化死亡率风险及可靠性调整后的比值比,并根据医院绩效五分位数评估患者和医院差异。我们使用分层回归模型来确定这些因素对死亡率的影响。
在805家医院中评估了72733例肝硬化入院病例。医院平均每年肝硬化病例数为90.4(范围25 - 828)。总体医院肝硬化死亡率为8.00%。医院调整后的死亡率比值比(aOR)范围为0.48至1.89。患者特征因医院死亡率aOR而有显著差异。住院时间平均为6.0±1.6天,且因医院绩效有显著差异(<0.001)。风险调整后死亡率的医院层面预测因素为较高的医疗补助病例组合(OR = 1.00, = 0.029)和 Licensed Practical Nurse(LPN)人员配备(OR = 1.02, = 0.015)。较高的肝硬化病例数(OR = 0.99, = 0.025)和肝移植项目状态(OR = 0.83, = 0.026)与生存率显著相关。在调整患者差异、时期和聚类效应后,医院间15.3%的差异可归因于医院特征差异。
医院特征在肝硬化死亡率差异中占很大比例。这些发现对肝病护理中的患者、医疗服务提供者以及医疗保健提供和住院医疗保健设计有若干启示。