Gedela Maheedhar, Kumar Vishesh, Shaikh Kashif Abbas, Stys Adam, Stys Tomasz
Department of Internal Medicine, University of South Dakota Sanford School of Medicine, Sioux Falls, SD, USA.
Sanford Cardiovascular Institute, University of South Dakota Sanford School of Medicine, Sioux Falls, SD, USA.
Case Rep Vasc Med. 2017;2017:8538149. doi: 10.1155/2017/8538149. Epub 2017 Mar 1.
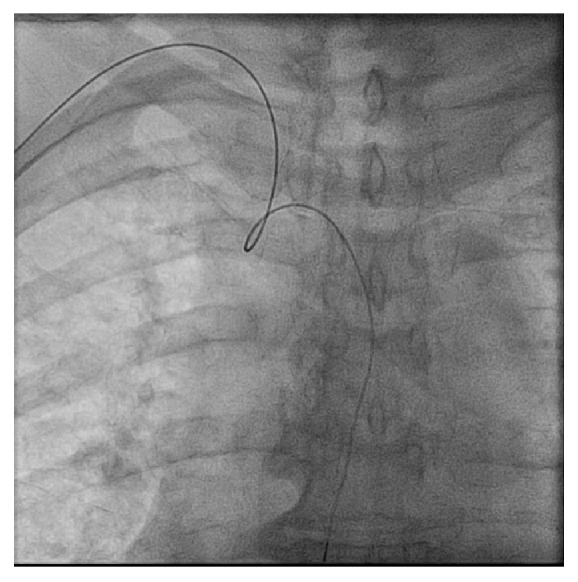
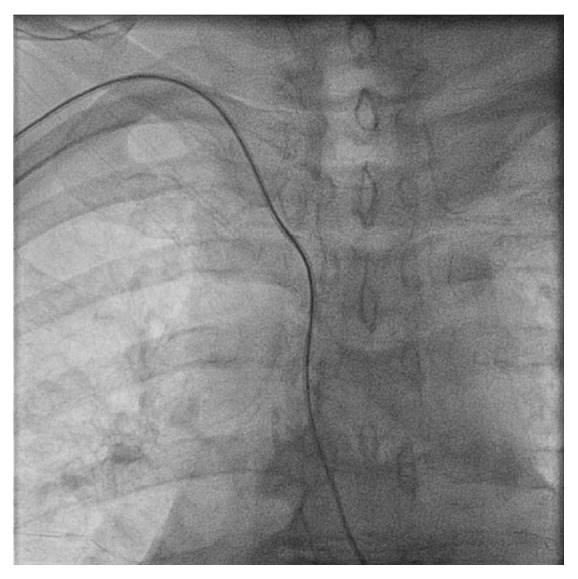
To report the resolution of bradycardia encountered during transradial cardiac catheterization through the catheter pullback technique in two cases. A 62-year-old male and an 81-year-old male underwent coronary angiogram to evaluate for coronary artery disease and as a result of positive stress test, respectively. Upon engagement of the FL 3.5 catheter into the ascending aorta through the transradial approach, the first case developed bradycardia with a heart rate of 39 beats per minute. The second case developed profound bradycardia with a heart rate of 25 beats per minute upon insertion of the 5 Fr FL 3.5 catheter near the right brachiocephalic trunk through the right radial access. Bradycardia can be subsided by removal of the catheter during catheter manipulation in patients undergoing transradial coronary angiogram if there is a suspicion of excessive stretching of aortic arch receptors and/or carotid sinus receptors.
报告两例经桡动脉心脏导管插入术中通过导管回撤技术解决心动过缓的情况。一名62岁男性和一名81岁男性分别因冠状动脉疾病评估和阳性负荷试验结果接受冠状动脉造影。在第一例中,通过经桡动脉途径将FL 3.5导管插入升主动脉时,出现心动过缓,心率为每分钟39次。在第二例中,通过右桡动脉入路将5 Fr FL 3.5导管插入右头臂干附近时,出现严重心动过缓,心率为每分钟25次。在经桡动脉冠状动脉造影的患者中,如果怀疑主动脉弓感受器和/或颈动脉窦感受器过度伸展,在导管操作过程中通过移除导管可使心动过缓缓解。