Beirer Marc, Banke Ingo J, Harrasser Norbert, Crönlein Moritz, Pförringer Dominik, Huber-Wagner Stefan, Biberthaler Peter, Kirchhoff Chlodwig
Department of Trauma Surgery, Klinikum rechts der Isar, Technical University of Munich, Ismaningerstr. 22, Munich, 81675, Germany.
Clinic of Orthopedics and Sports Orthopedics, Klinikum rechts der Isar, Technical University of Munich, Ismaningerstr. 22, Munich, 81675, Germany.
BMC Musculoskelet Disord. 2017 Mar 29;18(1):129. doi: 10.1186/s12891-017-1488-2.
Treatment of clavicular non- and malunion is still challenging. Current surgical procedures often result in frustrating functional outcome along with high-grade subjective impairment and increased rates of revision surgery. However, the combination of biological augmentation with vital bone graft and a biomechanically sufficient fixation system seems to be a promising concept of treatment.
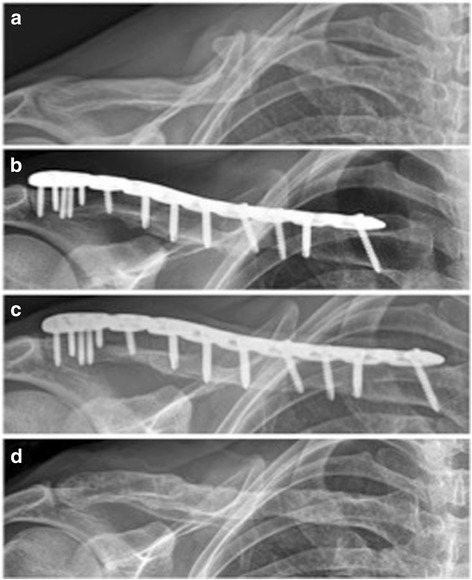
In this retrospective study, 14 patients with a mean age of 44 years (26-67 years) suffering from non-union (n = 11) and/or malunion (n = 3) of the clavicle were enrolled. All patients were surgically treated using an anatomical precontoured locking compression plate (LCP) and autologous iliac crest bone graft. Functional outcome was assessed using the age- and sex-specific relative Constant Score.
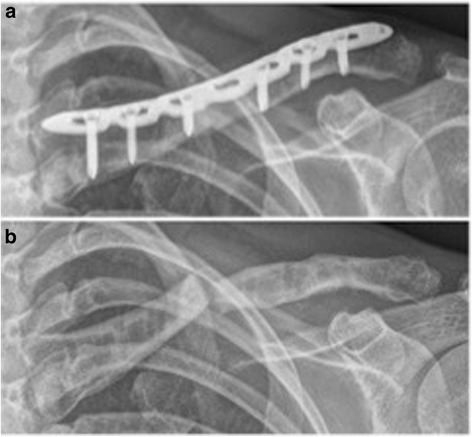
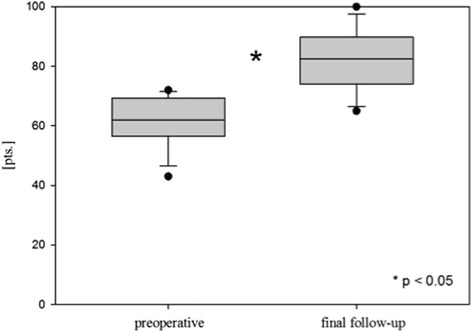
Mean follow-up was 27 months (range 12-44 months). The relative Constant Score significantly improved from preoperative 61 ± 8 (43-72) to 82 ± 10 (65-100) points at the final follow-up examination (p < 0.05). All patients showed bony union radiographically. One patient presented with a re-fracture of the clavicle nearly 3 years after revision surgery and 5 weeks after implant removal. Secondary fractures at the donor site of the anterior superior iliac spine were recorded in two patients.
Iliac crest bone graft and anatomic locking plate fixation allow for a safe and adequate stabilization and radiographical bony union in non- and malunions of the clavicle with a high degree of patient satisfaction. However, secondary fractures of the anterior superior iliac spine constitute relevant complications and the time of hardware removal should be considered carefully.
锁骨骨不连和畸形愈合的治疗仍然具有挑战性。目前的外科手术常常导致令人沮丧的功能结果,伴有严重的主观功能障碍以及翻修手术率增加。然而,生物增强与活性骨移植以及生物力学上足够的固定系统相结合似乎是一种有前景的治疗理念。
在这项回顾性研究中,纳入了14例平均年龄44岁(26 - 67岁)的锁骨骨不连(n = 11)和/或畸形愈合(n = 3)患者。所有患者均采用解剖预塑形锁定加压钢板(LCP)和自体髂嵴骨移植进行手术治疗。使用年龄和性别特异性相对Constant评分评估功能结果。
平均随访27个月(范围12 - 44个月)。相对Constant评分从术前的61±8(43 - 72)分显著提高至末次随访时的82±10(65 - 100)分(p < 0.05)。所有患者影像学检查均显示骨愈合。1例患者在翻修手术后近3年且取出植入物5周后出现锁骨再骨折。2例患者记录有髂前上棘供骨部位的二次骨折。
髂嵴骨移植和解剖锁定钢板固定可实现锁骨骨不连和畸形愈合的安全、充分稳定以及影像学骨愈合,患者满意度高。然而,髂前上棘二次骨折构成相关并发症,应仔细考虑取出内固定物的时机。