Otshudiema John O, Ndakala Nestor G, Mawanda Elande-Taty K, Tshapenda Gaston P, Kimfuta Jacques M, Nsibu Loupy-Régence N, Gueye Abdou S, Dee Jacob, Philen Rossanne M, Giese Coralie, Murrill Christopher S, Arthur Ray R, Kebela Benoit I
MMWR Morb Mortal Wkly Rep. 2017 Mar 31;66(12):335-338. doi: 10.15585/mmwr.mm6612a5.
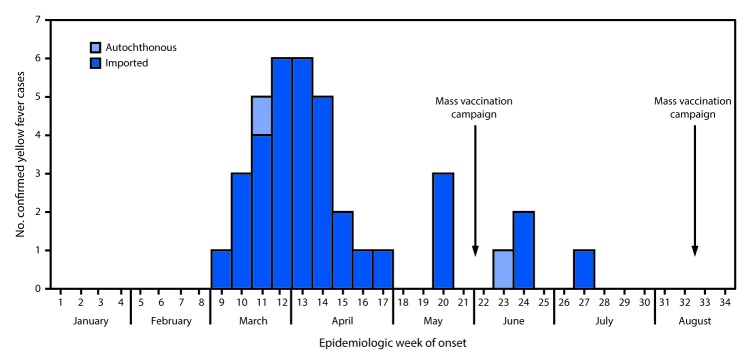
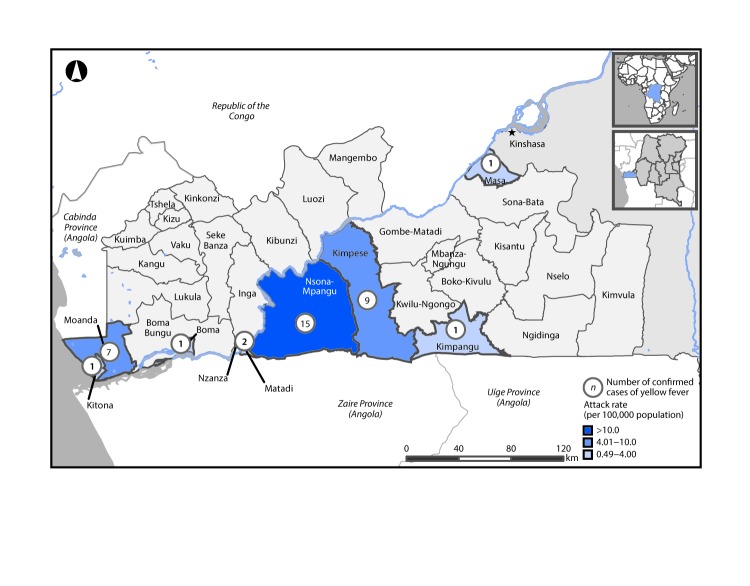
On April 23, 2016, the Democratic Republic of the Congo's (DRC's) Ministry of Health declared a yellow fever outbreak. As of May 24, 2016, approximately 90% of suspected yellow fever cases (n = 459) and deaths (45) were reported in a single province, Kongo Central Province, that borders Angola, where a large yellow fever outbreak had begun in December 2015. Two yellow fever mass vaccination campaigns were conducted in Kongo Central Province during May 25-June 7, 2016 and August 17-28, 2016. In June 2016, the DRC Ministry of Health requested assistance from CDC to control the outbreak. As of August 18, 2016, a total of 410 suspected yellow fever cases and 42 deaths were reported in Kongo Central Province. Thirty seven of the 393 specimens tested in the laboratory were confirmed as positive for yellow fever virus (local outbreak threshold is one laboratory-confirmed case of yellow fever). Although not well-documented for this outbreak, malaria, viral hepatitis, and typhoid fever are common differential diagnoses among suspected yellow fever cases in this region. Other possible diagnoses include Zika, West Nile, or dengue viruses; however, no laboratory-confirmed cases of these viruses were reported. Thirty five of the 37 cases of yellow fever were imported from Angola. Two-thirds of confirmed cases occurred in persons who crossed the DRC-Angola border at one market city on the DRC side, where ≤40,000 travelers cross the border each week on market day. Strategies to improve coordination between health surveillance and cross-border trade activities at land borders and to enhance laboratory and case-based surveillance and health border screening capacity are needed to prevent and control future yellow fever outbreaks.
2016年4月23日,刚果民主共和国(DRC)卫生部宣布爆发黄热病疫情。截至2016年5月24日,约90%的疑似黄热病病例(n = 459)和死亡病例(45例)报告来自与安哥拉接壤的单一省份——中刚果省,安哥拉于2015年12月开始爆发大规模黄热病疫情。2016年5月25日至6月7日以及8月17日至28日期间,在中刚果省开展了两次黄热病大规模疫苗接种活动。2016年6月,刚果民主共和国卫生部请求美国疾病控制与预防中心(CDC)协助控制疫情。截至2016年8月18日,中刚果省共报告410例疑似黄热病病例和42例死亡病例。在实验室检测的393份样本中,有37份被确认为黄热病病毒阳性(当地疫情爆发阈值为1例实验室确诊的黄热病病例)。尽管此次疫情的记录并不完善,但疟疾、病毒性肝炎和伤寒热是该地区疑似黄热病病例中常见的鉴别诊断疾病。其他可能的诊断包括寨卡病毒、西尼罗河病毒或登革热病毒;然而,尚未报告这些病毒的实验室确诊病例。37例黄热病病例中有35例是从安哥拉输入的。三分之二的确诊病例发生在刚果民主共和国一侧的一个边境市场城市,每周集市日有≤40,000名旅行者从这里跨境。需要采取策略来改善陆地边境卫生监测与跨境贸易活动之间的协调,加强实验室监测和基于病例的监测以及卫生边境筛查能力,以预防和控制未来的黄热病疫情。