Wen Joanne C, Reina-Torres Ester, Sherwood Joseph M, Challa Pratap, Liu Katy C, Li Guorong, Chang Jason Y H, Cousins Scott W, Schuman Stefanie G, Mettu Priyatham S, Stamer W Daniel, Overby Darryl R, Allingham R Rand
Department of Ophthalmology, University of Washington, Seattle, Washington, United States 2Department of Ophthalmology, Duke University Eye Center, Durham, North Carolina, United States.
Department of Bioengineering, Imperial College London, London, United Kingdom.
Invest Ophthalmol Vis Sci. 2017 Mar 1;58(3):1893-1898. doi: 10.1167/iovs.16-20786.
We assess the effect of intravitreal anti-VEGF injections on tonographic outflow facility.
Patients with age-related macular degeneration who had received unilateral intravitreal anti-VEGF injections were recruited into two groups, those with ≤10 and those with ≥20 total anti-VEGF injections. Intraocular pressure and tonographic outflow facility of injected and uninjected fellow eyes were measured and compared between groups. Risk factors for development of reduced outflow facility also were assessed.
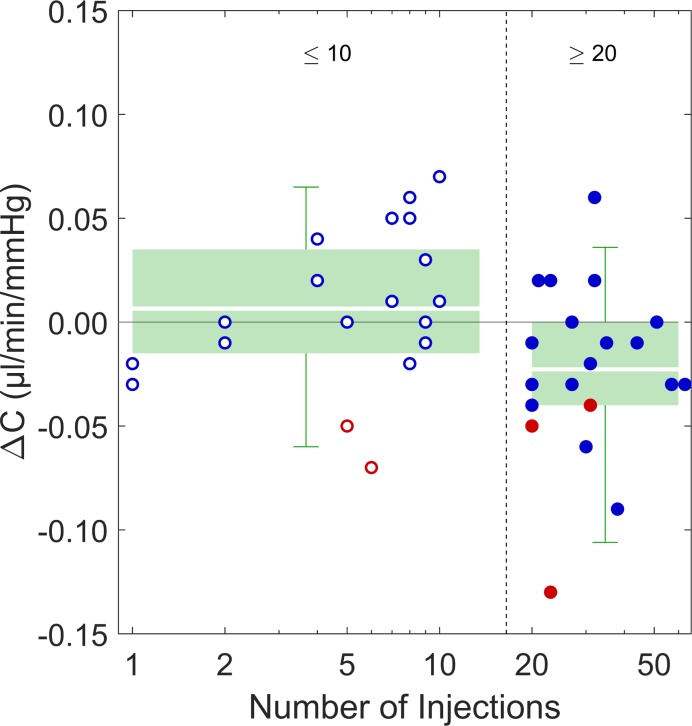
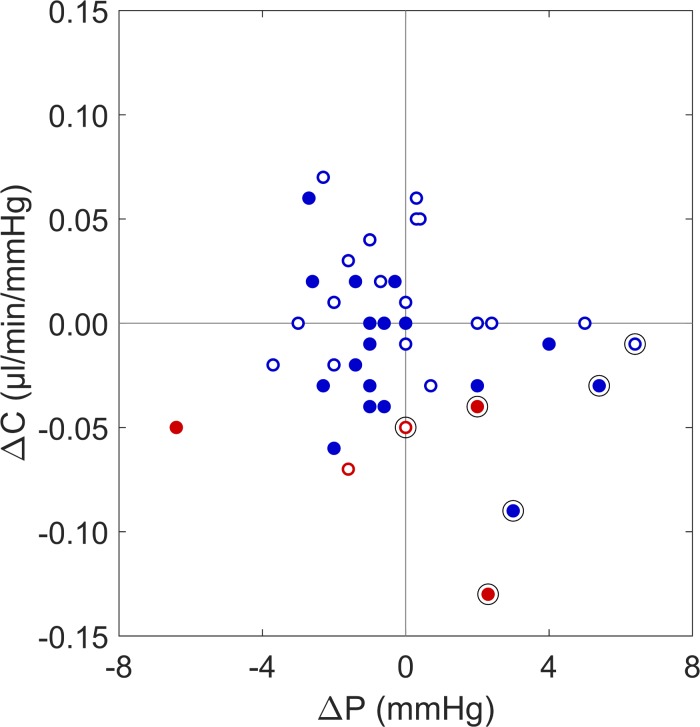
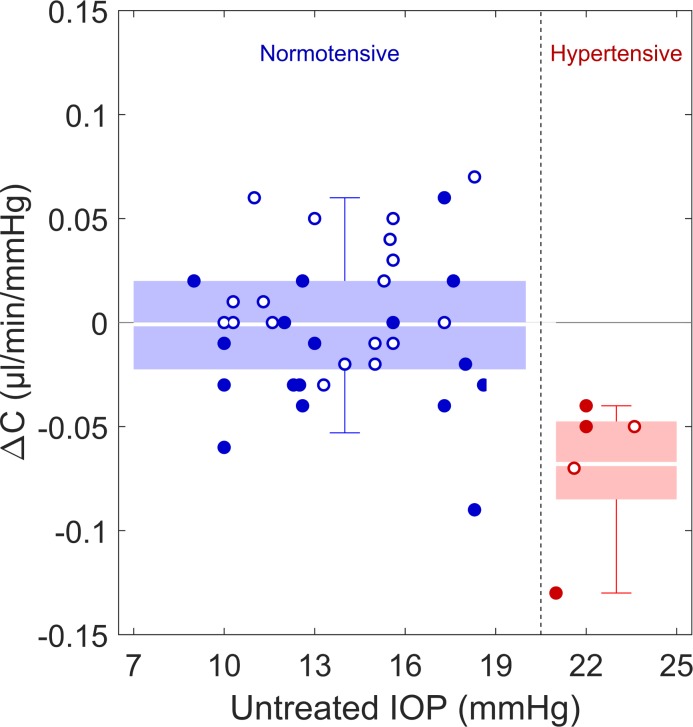
Outflow facility was 12% lower in the injected eyes of patients who received ≥20 anti-VEGF injections, compared to contralateral uninjected eyes (P = 0.02). In contrast, there was no facility reduction for patients with ≤10 anti-VEGF injections (P = 0.4). In patients with ocular hypertension in the uninjected eye (IOP > 21 mm Hg, n = 5), the outflow facility of injected eyes was on average 46% lower (P = 0.01) than in the uninjected fellow eyes. This was significantly greater than the difference observed in patients with IOP ≤ 21 mm Hg in the uninjected eye (P = 2 × 10-4). In patients with ocular hypertension in the injected eye (n = 6) the differences in facility and IOP between contralateral eyes were significantly greater than in patients with IOP ≤ 21 mm Hg in the injected eye (P = 2 × 10-4 and P = 7 × 10-4, respectively).
Chronic anti-VEGF injections significantly reduce outflow facility in patients with AMD. The greatest facility reduction is observed in patients with baseline ocular hypertension. Ophthalmologists who administer anti-VEGF injections should be aware of these findings and monitor patients closely for changes in IOP or evidence of glaucoma, especially in those with pre-existing ocular hypertension.
我们评估玻璃体内抗血管内皮生长因子(VEGF)注射对眼压描记流出易度的影响。
招募接受过单侧玻璃体内抗VEGF注射的年龄相关性黄斑变性患者,分为两组,分别是抗VEGF注射总量≤10次和≥20次的患者。测量并比较注射眼和未注射对侧眼的眼压及眼压描记流出易度。还评估了流出易度降低的危险因素。
接受≥20次抗VEGF注射的患者,其注射眼的流出易度比未注射的对侧眼低12%(P = 0.02)。相比之下,抗VEGF注射≤10次的患者流出易度没有降低(P = 0.4)。未注射眼患有高眼压(眼压>21 mmHg,n = 5)的患者,其注射眼的流出易度平均比未注射的对侧眼低46%(P = 0.01)。这显著大于未注射眼眼压≤21 mmHg的患者中观察到的差异(P = 2×10⁻⁴)。注射眼患有高眼压(n = 6)的患者,其对侧眼在流出易度和眼压方面的差异显著大于注射眼眼压≤21 mmHg的患者(分别为P = 2×10⁻⁴和P = 7×10⁻⁴)。
慢性抗VEGF注射会显著降低年龄相关性黄斑变性患者的流出易度。在基线患有高眼压的患者中观察到流出易度降低最为明显。进行抗VEGF注射的眼科医生应知晓这些发现,并密切监测患者眼压变化或青光眼迹象,尤其是那些已有高眼压的患者。