Department of Cardiology, University Medical Center Groningen University of Groningen, The Netherlands.
Heart Failure Research Center, Academic Medical Center, Amsterdam, The Netherlands.
J Am Heart Assoc. 2017 Mar 30;6(4):e003989. doi: 10.1161/JAHA.116.003989.
Biomarkers may help us to unravel differences in the underlying pathophysiology between heart failure (HF) patients with a reduced ejection fraction (HFrEF) and a preserved ejection fraction (HFpEF). Therefore, we compared biomarker profiles to characterize pathophysiological differences between patients with HFrEF and HFpEF.
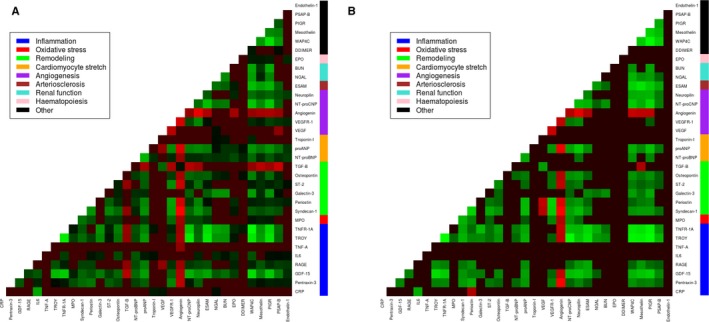
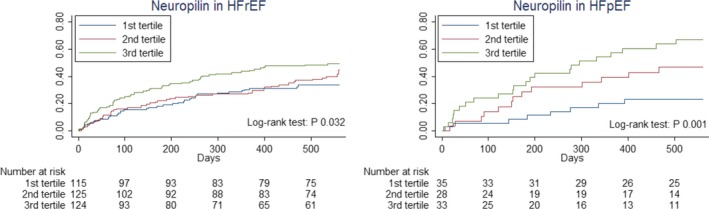
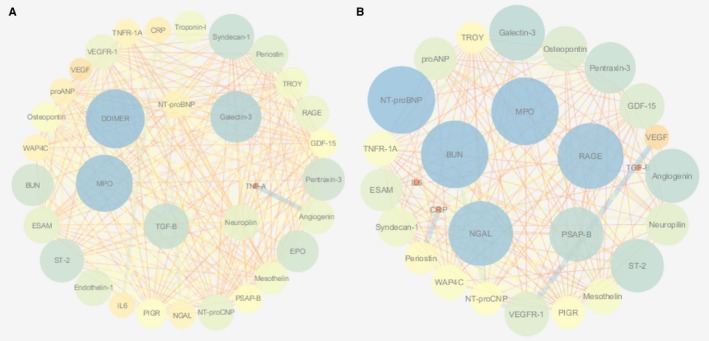
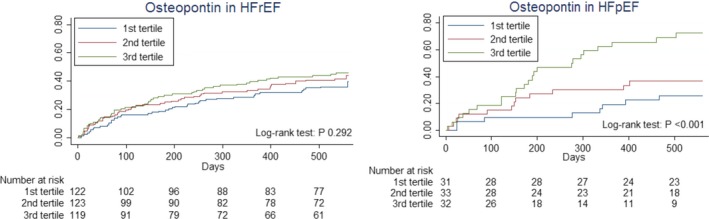
We retrospectively analyzed 33 biomarkers from different pathophysiological domains (inflammation, oxidative stress, remodeling, cardiac stretch, angiogenesis, arteriosclerosis, and renal function) in 460 HF patients (21% HFpEF, left ventricular ejection fraction ≥45%) measured at discharge after hospitalization for acute HF. The association between these markers and the occurrence of all-cause mortality and/or HF-related rehospitalizations at 18 months was compared between patients with HFrEF and HFpEF. Patients were 70.6±11.4 years old and 37.4% were female. Patients with HFpEF were older, more often female, and had a higher systolic blood pressure. Levels of high-sensitive C-reactive protein were significantly higher in HFpEF, while levels of pro-atrial-type natriuretic peptide and N-terminal pro-brain natriuretic peptide were higher in HFrEF. Linear regression followed by network analyses revealed prominent inflammation and angiogenesis-associated interactions in HFpEF and mainly cardiac stretch-associated interactions in HFrEF. The angiogenesis-specific marker, neuropilin and the remodeling-specific marker, osteopontin were predictive for all-cause mortality and/or HF-related rehospitalizations at 18 months in HFpEF, but not in HFrEF ( for interaction <0.05).
In HFpEF, inflammation and angiogenesis-mediated interactions are predominantly observed, while stretch-mediated interactions are found in HFrEF. The remodeling marker osteopontin and the angiogenesis marker neuropilin predicted outcome in HFpEF, but not in HFrEF.
生物标志物可能有助于我们揭示射血分数降低的心力衰竭(HFrEF)和射血分数保留的心力衰竭(HFpEF)患者潜在病理生理学差异。因此,我们比较了生物标志物谱,以描述 HFrEF 和 HFpEF 患者之间的病理生理学差异。
我们回顾性分析了 460 例因急性心力衰竭住院后出院时测量的 33 种来自不同病理生理领域(炎症、氧化应激、重构、心脏拉伸、血管生成、动脉硬化和肾功能)的生物标志物(21%HFpEF,左心室射血分数≥45%)。比较 HFrEF 和 HFpEF 患者之间这些标志物与 18 个月全因死亡率和/或心力衰竭相关再住院的发生之间的关联。患者的年龄为 70.6±11.4 岁,37.4%为女性。HFpEF 患者年龄较大,女性更多,收缩压更高。HFpEF 患者的高敏 C 反应蛋白水平明显较高,而 HFrEF 患者的前心房型利钠肽和 N 末端脑利钠肽前体水平较高。线性回归后网络分析显示,HFpEF 中主要存在炎症和血管生成相关的相互作用,而 HFrEF 中主要存在心脏拉伸相关的相互作用。血管生成特异性标志物神经纤毛蛋白和重构特异性标志物骨桥蛋白可预测 HFpEF 患者 18 个月时的全因死亡率和/或心力衰竭相关再住院,但不能预测 HFrEF 患者(交互作用<0.05)。
在 HFpEF 中,观察到主要是炎症和血管生成介导的相互作用,而在 HFrEF 中则发现了拉伸介导的相互作用。重构标志物骨桥蛋白和血管生成标志物神经纤毛蛋白可预测 HFpEF 患者的预后,但不能预测 HFrEF 患者的预后。