Horne Kerry L, Packington Rebecca, Monaghan John, Reilly Timothy, Selby Nicholas M
Department of Renal Medicine, Derby Teaching Hospitals NHS Foundation Trust, Derby, UK.
Department of Chemical Pathology, Derby Teaching Hospitals NHS Foundation Trust, Derby, UK.
BMJ Open. 2017 Mar 29;7(3):e015316. doi: 10.1136/bmjopen-2016-015316.
Using a prospective study design, we aimed to characterise the effect of acute kidney injury (AKI) on long-term changes in renal function in a general hospital population.
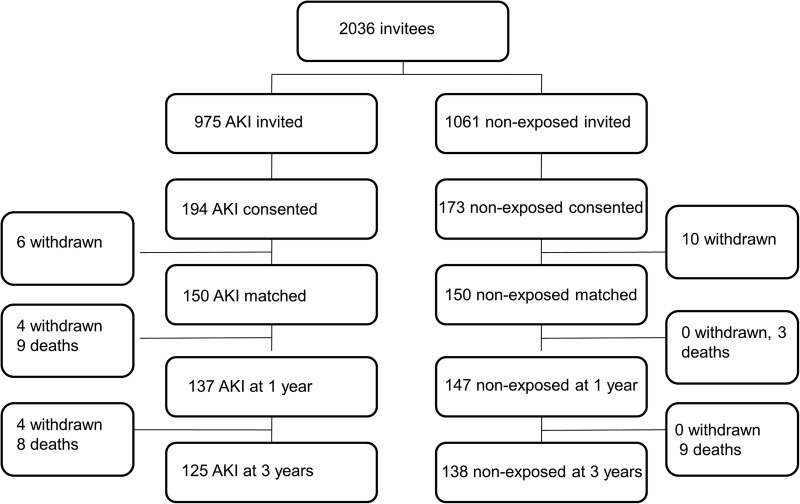
Hospitalised patients with AKI (exposed) and hospitalised patients without AKI (non-exposed), recruited at 3 months after hospital admission.
Prospective, matched parallel group cohort study, in which renal function and proteinuria were measured at 3 months, 1 year and 3 years.
Single UK centre.
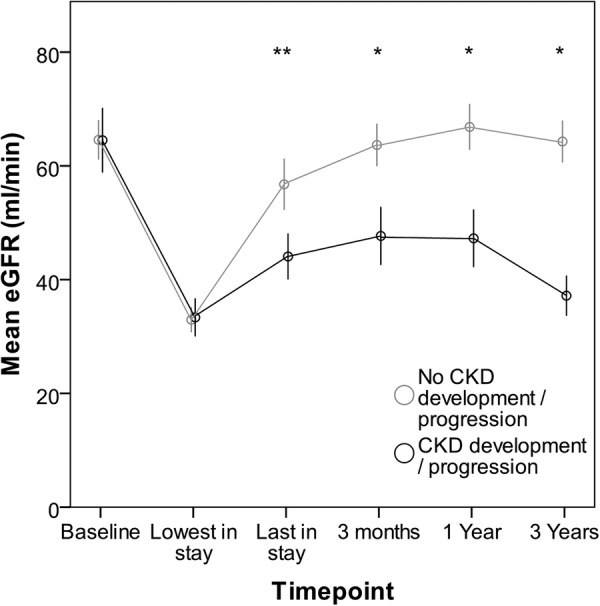
Clinical end points at 3 years were comparison of the following variables between exposed and non-exposed groups: renal function, prevalence of proteinuria and albuminuria and chronic kidney disease (CKD) progression/development at each time point. CKD progression was defined as a decrease in the estimated glomerular filtration rate (eGFR) of ≥25% associated with a decline in eGFR stage.
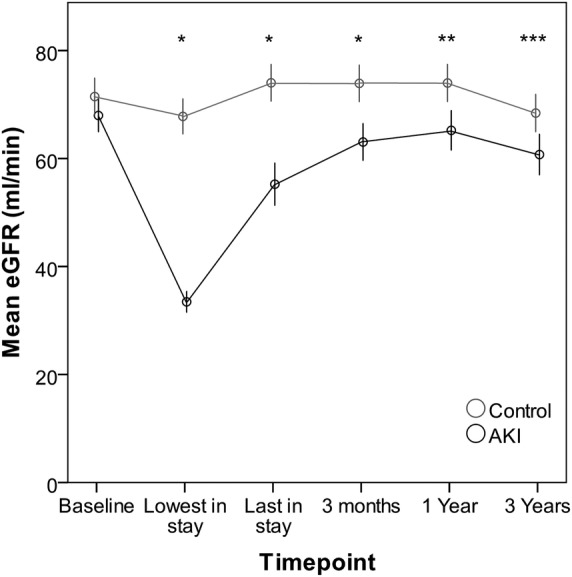
300 exposed and non-exposed patients were successfully matched 1:1 for age and baseline renal function; 70% of the exposed group had AKI stage 1. During follow-up, the AKI group had lower eGFR than non-exposed patients at each time point. At 3 years, the mean eGFR was 60.7±21 mL/min/1.73 m in the AKI group compared with 68.4±21 mL/min/1.73 m in the non-exposed group, p=0.003. CKD development or progression at 3 years occurred in 30 (24.6%) of the AKI group compared with 10 (7.5%) of the non-exposed group, p<0.001. Albuminuria was more common in the AKI group, and increased with AKI severity. Factors independently associated with CKD development/progression after AKI were non-recovery at 90 days, male gender, diabetes and recurrent AKI.
AKI is associated with deterioration in renal function to 3 years, even in an unselected population with predominantly AKI stage 1. Non-recovery from AKI is an important factor determining long-term outcome.
采用前瞻性研究设计,我们旨在描述急性肾损伤(AKI)对综合医院人群肾功能长期变化的影响。
住院的AKI患者(暴露组)和无AKI的住院患者(非暴露组),在入院3个月后招募。
前瞻性、匹配平行组队列研究,在3个月、1年和3年时测量肾功能和蛋白尿。
英国单一中心。
3年时的临床终点是比较暴露组和非暴露组之间的以下变量:肾功能、蛋白尿和白蛋白尿的患病率以及每个时间点慢性肾脏病(CKD)的进展/发生情况。CKD进展定义为估计肾小球滤过率(eGFR)下降≥25%且eGFR分期下降。
300例暴露组和非暴露组患者在年龄和基线肾功能方面成功进行了1:1匹配;暴露组70%为1期AKI。在随访期间,AKI组在每个时间点的eGFR均低于非暴露组患者。3年时,AKI组的平均eGFR为60.7±21 mL/min/1.73 m²,而非暴露组为68.4±21 mL/min/1.73 m²,p = 0.003。3年时,AKI组有30例(24.6%)发生CKD进展或新发,而非暴露组有10例(7.5%),p < 0.001。白蛋白尿在AKI组更常见,并随AKI严重程度增加。AKI后与CKD进展/新发独立相关的因素包括90天时未恢复、男性、糖尿病和复发性AKI。
即使在以1期AKI为主的未选择人群中,AKI也与3年时的肾功能恶化相关。AKI未恢复是决定长期预后的重要因素。