James Matthew T, Grams Morgan E, Woodward Mark, Elley C Raina, Green Jamie A, Wheeler David C, de Jong Paul, Gansevoort Ron T, Levey Andrew S, Warnock David G, Sarnak Mark J
Department of Medicine, University of Calgary, Calgary, Alberta, Canada; Department of Community Health Sciences, University of Calgary, Calgary, Alberta, Canada.
Johns Hopkins Bloomberg School of Public Health, Baltimore, MD.
Am J Kidney Dis. 2015 Oct;66(4):602-12. doi: 10.1053/j.ajkd.2015.02.338. Epub 2015 May 11.
Diabetes mellitus and hypertension are risk factors for acute kidney injury (AKI). Whether estimated glomerular filtration rate (eGFR) and urine albumin-creatinine ratio (ACR) remain risk factors for AKI in the presence and absence of these conditions is uncertain.
Meta-analysis of cohort studies.
SETTING & POPULATION: 8 general-population (1,285,045 participants) and 5 chronic kidney disease (CKD; 79,519 participants) cohorts.
Cohorts participating in the CKD Prognosis Consortium.
Diabetes and hypertension status, eGFR by the 2009 CKD Epidemiology Collaboration creatinine equation, urine ACR, and interactions.
Hospitalization with AKI, using Cox proportional hazards models to estimate HRs of AKI and random-effects meta-analysis to pool results.
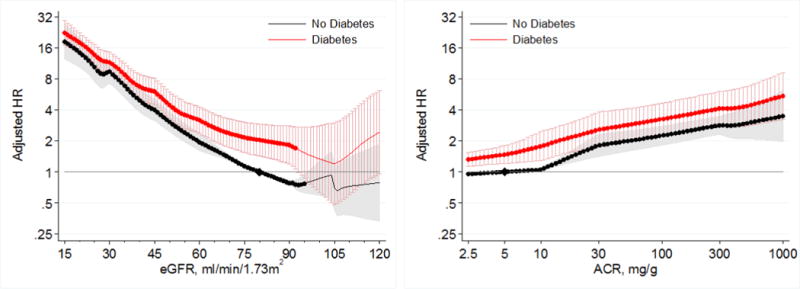
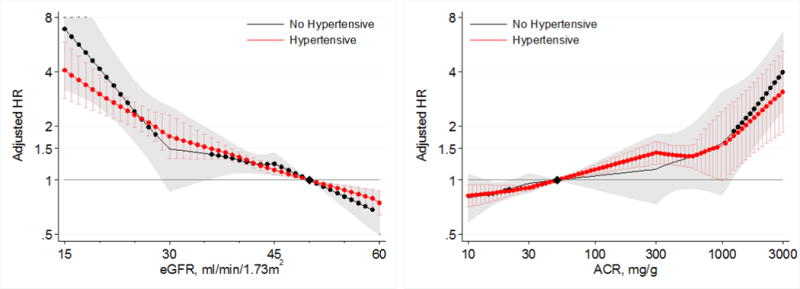
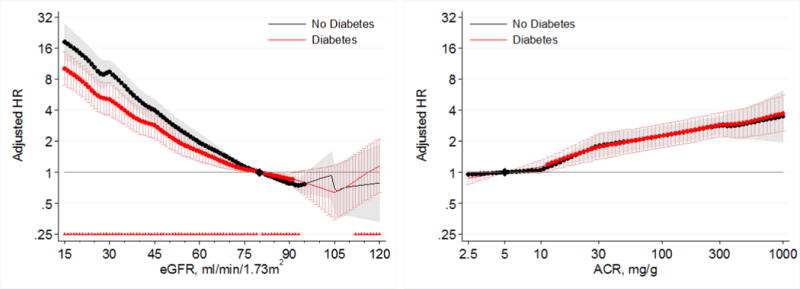
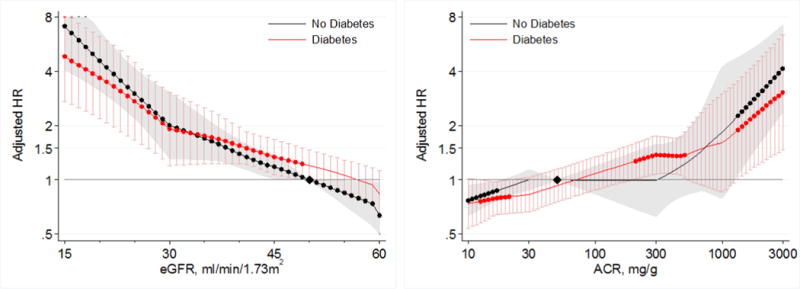
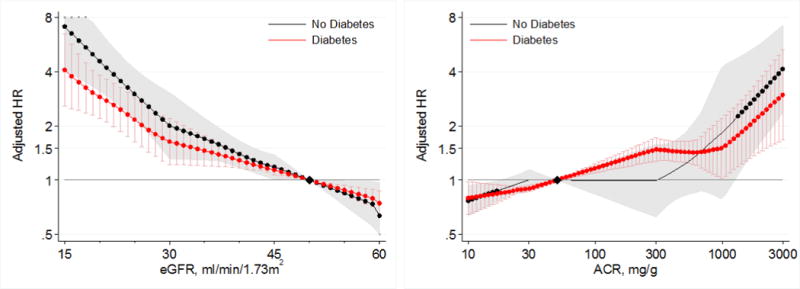
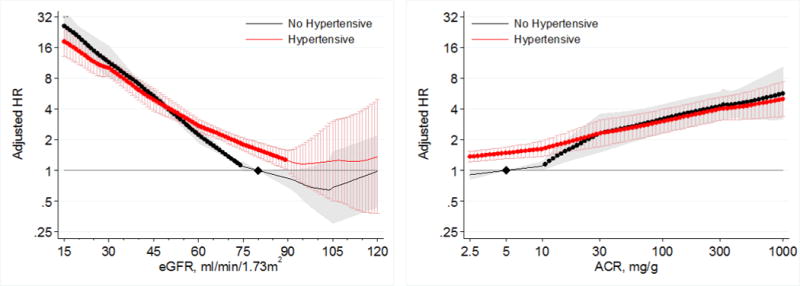
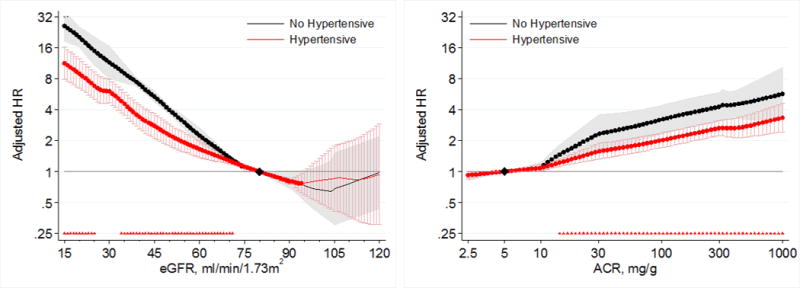
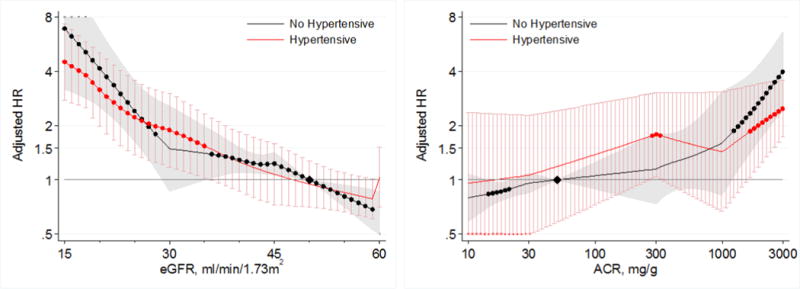
During a mean follow-up of 4 years, there were 16,480 episodes of AKI in the general-population and 2,087 episodes in the CKD cohorts. Low eGFRs and high ACRs were associated with higher risks of AKI in individuals with or without diabetes and with or without hypertension. When compared to a common reference of eGFR of 80mL/min/1.73m(2) in nondiabetic patients, HRs for AKI were generally higher in diabetic patients at any level of eGFR. The same was true for diabetic patients at all levels of ACR compared with nondiabetic patients. The risk gradient for AKI with lower eGFRs was greater in those without diabetes than with diabetes, but similar with higher ACRs in those without versus with diabetes. Those with hypertension had a higher risk of AKI at eGFRs>60mL/min/1.73m(2) than those without hypertension. However, risk gradients for AKI with both lower eGFRs and higher ACRs were greater for those without than with hypertension.
AKI identified by diagnostic code.
Lower eGFRs and higher ACRs are associated with higher risks of AKI among individuals with or without either diabetes or hypertension.
糖尿病和高血压是急性肾损伤(AKI)的危险因素。在存在或不存在这些情况时,估计肾小球滤过率(eGFR)和尿白蛋白肌酐比值(ACR)是否仍是AKI的危险因素尚不确定。
队列研究的荟萃分析。
8个普通人群队列(1285045名参与者)和5个慢性肾脏病(CKD)队列(79519名参与者)。
参与CKD预后联盟的队列。
糖尿病和高血压状态、根据2009年CKD流行病学协作组肌酐方程得出的eGFR、尿ACR以及相互作用。
因AKI住院,使用Cox比例风险模型估计AKI的风险比(HR),并采用随机效应荟萃分析汇总结果。
在平均4年的随访期间,普通人群中有16480例AKI发作,CKD队列中有2087例发作。低eGFR和高ACR与有或无糖尿病、有或无高血压个体的AKI风险较高相关。与非糖尿病患者eGFR为80mL/min/1.73m²的常见参考值相比,在任何eGFR水平下,糖尿病患者发生AKI的HR通常更高。在所有ACR水平下,糖尿病患者与非糖尿病患者相比也是如此。eGFR较低时,非糖尿病患者AKI的风险梯度大于糖尿病患者,但ACR较高时,非糖尿病患者与糖尿病患者的情况相似。eGFR>60mL/min/1.73m²时,高血压患者发生AKI的风险高于无高血压者。然而,eGFR较低和ACR较高时,无高血压者AKI的风险梯度大于有高血压者。
通过诊断代码识别AKI。
无论有无糖尿病或高血压,较低的eGFR和较高的ACR均与个体发生AKI的较高风险相关。