Rodrigo Gustavo J, Price David, Anzueto Antonio, Singh Dave, Altman Pablo, Bader Giovanni, Patalano Francesco, Fogel Robert, Kostikas Konstantinos
Departamento de Emergencia, Hospital Central de las Fuerzas Armadas, Montevideo, Uruguay.
Academic Primary Care, Division of Applied Health Sciences, University of Aberdeen, Aberdeen, Scotland, UK; Observational and Pragmatic Research Institute, Singapore.
Int J Chron Obstruct Pulmon Dis. 2017 Mar 17;12:907-922. doi: 10.2147/COPD.S130482. eCollection 2017.
Randomized controlled trials (RCTs) indicate that long-acting bronchodilator combinations, such as β-agonist (LABA)/muscarinic antagonist (LAMA), have favorable efficacy compared with commonly used COPD treatments. The objective of this analysis was to compare the efficacy and safety of LABA/LAMA with LAMA or LABA/inhaled corticosteroid (ICS) in adults with stable moderate-to-very-severe COPD.
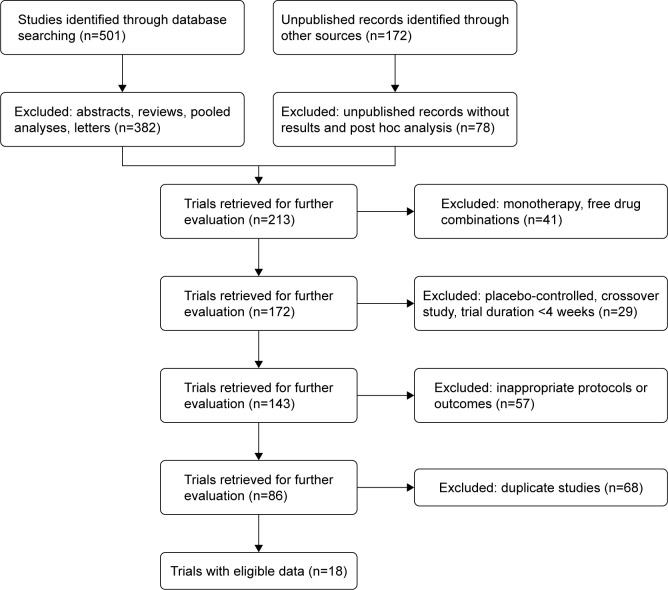
This systematic review and meta-analysis (PubMed/MEDLINE, Embase, Cochrane Library and clinical trial/manufacturer databases) included RCTs comparing ≥12 weeks' LABA/LAMA treatment with LAMA and/or LABA/ICS (approved doses only). Eligible studies were independently selected by two authors using predefined data fields; the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were followed.
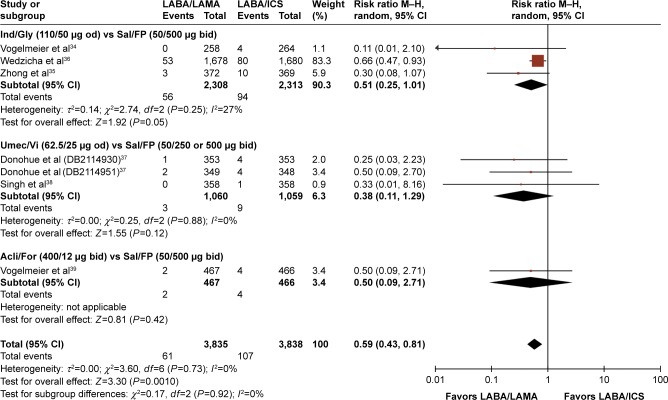
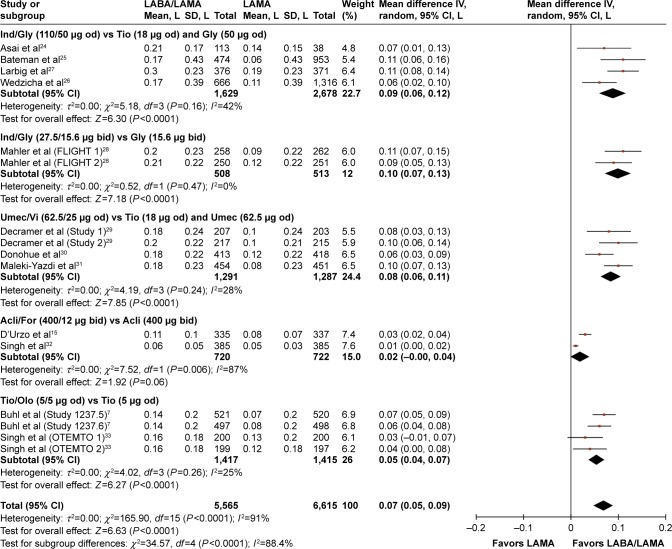
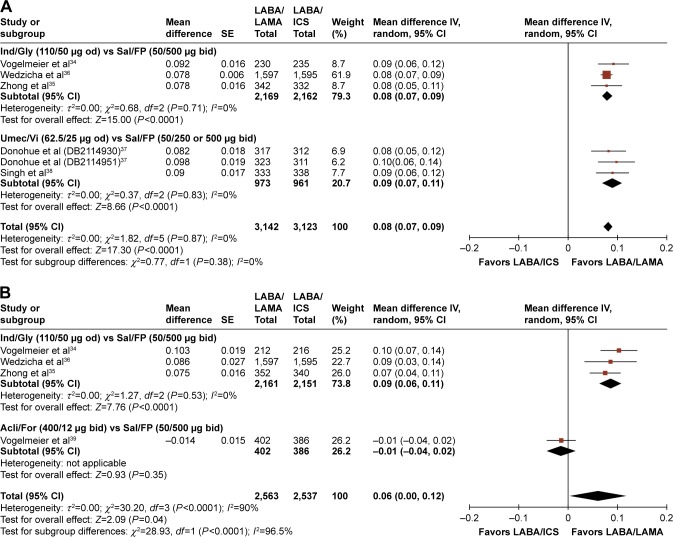
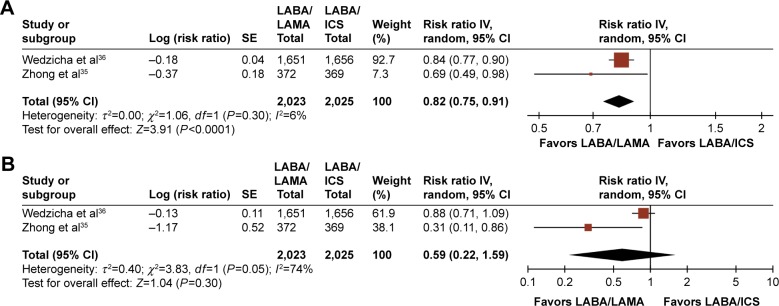
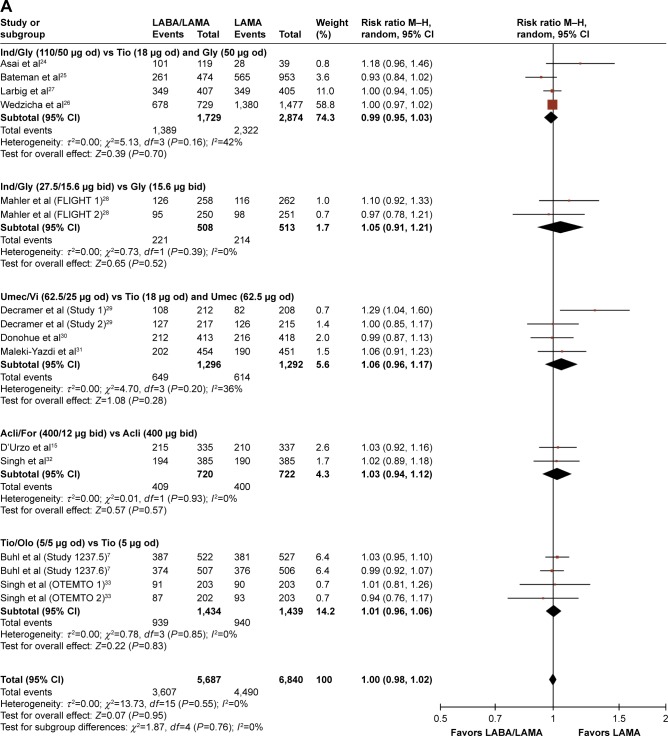
Eighteen studies (23 trials) were eligible (N=20,185). LABA/LAMA significantly improved trough forced expiratory volume in 1 second (FEV) from baseline to week 12 versus both LAMA and LABA/ICS (0.07 L and 0.08 L, <0.0001), with patients more likely to achieve clinically important improvements in FEV of >100 mL (risk ratio [RR]: 1.33, 95% confidence interval [CI]: [1.20, 1.46] and RR: 1.44, 95% CI: [1.33, 1.56], respectively, the number needed to treat being eight and six, respectively). LABA/LAMA improved transitional dyspnea index and St George's Respiratory Questionnaire scores at week 12 versus LAMA (both <0.0001), but not versus LABA/ICS, and reduced rescue medication use versus both (<0.0001 and =0.001, respectively). LABA/LAMA significantly reduced moderate/severe exacerbation rate compared with LABA/ICS (RR 0.82, 95% CI: [0.75, 0.91]). Adverse event (AE) incidence was no different for LABA/LAMA versus LAMA treatment, but it was lower versus LABA/ICS (RR 0.94, 95% CI: [0.89, 0.99]), including a lower pneumonia risk (RR 0.59, 95% CI: [0.43, 0.81]). LABA/LAMA presented a lower risk for withdrawals due to lack of efficacy versus LAMA (RR: 0.66, 95% CI: [0.51, 0.87]) and due to AEs versus LABA/ICS (RR: 0.83, 95% CI: [0.69, 0.99]).
The greater efficacy and comparable safety profiles observed with LABA/LAMA combinations versus LAMA or LABA/ICS support their potential role as first-line treatment options in COPD. These findings are of direct relevance to clinical practice because we included all currently available LABA/LAMAs and comparators, only at doses approved for clinical use.
随机对照试验(RCT)表明,长效支气管扩张剂组合,如β受体激动剂(LABA)/毒蕈碱拮抗剂(LAMA),与常用的慢性阻塞性肺疾病(COPD)治疗方法相比具有良好的疗效。本分析的目的是比较LABA/LAMA与LAMA或LABA/吸入性糖皮质激素(ICS)在稳定的中度至重度COPD成人患者中的疗效和安全性。
本系统评价和荟萃分析(PubMed/MEDLINE、Embase、Cochrane图书馆和临床试验/制造商数据库)纳入了比较≥12周LABA/LAMA治疗与LAMA和/或LABA/ICS(仅批准剂量)的RCT。符合条件的研究由两名作者使用预定义的数据字段独立选择;遵循系统评价和荟萃分析的首选报告项目指南。
18项研究(23项试验)符合条件(N=20185)。与LAMA和LABA/ICS相比,LABA/LAMA在第12周时显著改善了从基线开始的1秒用力呼气容积(FEV)(分别为0.07L和0.08L,<0.0001),患者更有可能在FEV方面实现>100mL的临床重要改善(风险比[RR]:1.33,95%置信区间[CI]:[1.20,1.46];RR:1.44,95%CI:[1.33,1.56],治疗所需人数分别为8和6)。与LAMA相比,LABA/LAMA在第12周时改善了过渡性呼吸困难指数和圣乔治呼吸问卷评分(均<0.0001),但与LABA/ICS相比无差异,并且与两者相比减少了急救药物的使用(分别为<0.0001和=0.001)。与LABA/ICS相比,LABA/LAMA显著降低了中度/重度急性加重率(RR 0.82,95%CI:[0.75,0.91])。LABA/LAMA与LAMA治疗相比不良事件(AE)发生率无差异,但与LABA/ICS相比更低(RR 0.94,95%CI:[0.89,0.99]),包括更低的肺炎风险(RR 0.59,95%CI:[0.43,0.81])。与LAMA相比,LABA/LAMA因缺乏疗效而停药的风险更低(RR:0.66,95%CI:[0.51,0.87]),与LABA/ICS相比因AE停药的风险更低(RR:0.83,95%CI:[0.69,0.99])。
与LAMA或LABA/ICS相比,LABA/LAMA组合具有更高的疗效和相当的安全性,支持其作为COPD一线治疗选择的潜在作用。这些发现与临床实践直接相关,因为我们纳入了所有目前可用的LABA/LAMA和对照药物,且仅采用临床批准剂量。