Gerotziafas Grigoris T, Van Dreden Patrick, Mathieu d'Argent Emmanuelle, Lefkou Eleftheria, Grusse Matthieu, Comtet Marjorie, Sangare Rabiatou, Ketatni Hela, Larsen Annette K, Elalamy Ismail
Cancer Biology and Therapeutics, Centre de Recherche Saint-Antoine, Institut National de la Santé et de la Recherche Médicale (INSERM) U938 and Université Pierre et Marie Curie (UPMC), Sorbonne Universities, Paris, France.
Service d'Hématologie Biologique, Hôpital Tenon, Hôpitaux Universitaires Est Parisien, Assistance Publique Hôpitaux de Paris, 4, rue de la Chine, Paris, Cedex 20 France.
Thromb J. 2017 Mar 28;15:9. doi: 10.1186/s12959-017-0131-7. eCollection 2017.
Blood coagulation plays a crucial role in the blastocyst implantation process and its alteration may be related to in vitro fertilization (IVF) failure. We conducted a prospective observational longitudinal study in women eligible for IVF to explore the association between alterations of coagulation with the IVF outcome and to identify the biomarkers of hypercoagulability which are related with this outcome.
Thirty-eight women eligible for IVF (IVF-group) and 30 healthy, age-matched women (control group) were included. In the IVF-group, blood was collected at baseline, 5-8 days after administration of gonadotropin-releasing hormone agonist (GnRH), before and two weeks after administration of human follicular stimulating hormone (FSH). Pregnancy was monitored by measurement of HCG performed 15 days after embryo transfer. Thrombin generation (TG), minimal tissue factor-triggered whole blood thromboelastometry (ROTEM®), procoagulant phospholipid clotting time (Procoag-PPL®), thrombomodulin (TMa), tissue factor activity (TFa), factor VIII (FVIII), factor von Willebrand (FvW), D-Dimers and fibrinogen were assessed at each time point.
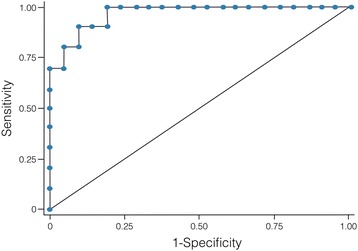
Positive IVF occurred in 15 women (40%). At baseline, the IVF-group showed significantly increased TG, TFa and TMa and significantly shorter Procoag-PPL versus the control group. After initiation of hormone treatment TG was significantly higher in the IVF-positive as compared to the IVF-negative group. At all studied points, the Procoag-PPL was significantly shorter and the levels of TFa were significantly higher in the IVF-negative group compared to the IVF-positive one. The D-Dimers were higher in the IVF negative as compared to IVF positive group. Multivariate analysis retained the Procoag-PPL and TG as predictors for the IVF outcome.
Diagnosis of women with hypercoagulability and their stratification to risk of IVF failure using a model based on the Procoag-PPL and TG is a feasible strategy for the optimization of IVF efficiency that needs to be validated in prospective trials.
血液凝固在囊胚着床过程中起着关键作用,其改变可能与体外受精(IVF)失败有关。我们对符合IVF条件的女性进行了一项前瞻性观察性纵向研究,以探讨凝血改变与IVF结局之间的关联,并确定与该结局相关的高凝生物标志物。
纳入38名符合IVF条件的女性(IVF组)和30名年龄匹配的健康女性(对照组)。在IVF组中,在基线、促性腺激素释放激素激动剂(GnRH)给药后5 - 8天、人卵泡刺激素(FSH)给药前和给药后两周采集血液。在胚胎移植后15天通过检测HCG监测妊娠情况。在每个时间点评估凝血酶生成(TG)、最小组织因子触发的全血血栓弹力图(ROTEM®)、促凝磷脂凝血时间(Procoag-PPL®)、血栓调节蛋白(TMa)、组织因子活性(TFa)、因子VIII(FVIII)、血管性血友病因子(FvW)、D-二聚体和纤维蛋白原。
15名女性(40%)IVF成功。在基线时,与对照组相比,IVF组的TG、TFa和TMa显著升高,Procoag-PPL显著缩短。激素治疗开始后,IVF阳性组的TG显著高于IVF阴性组。在所有研究时间点,与IVF阳性组相比,IVF阴性组的Procoag-PPL显著缩短,TFa水平显著升高。IVF阴性组的D-二聚体高于IVF阳性组。多变量分析保留Procoag-PPL和TG作为IVF结局的预测指标。
使用基于Procoag-PPL和TG的模型对高凝女性进行诊断并将其分层为IVF失败风险,是优化IVF效率的可行策略,需要在前瞻性试验中进行验证。