Layland Jamie, Rauhalammi Samuli, Lee Matthew M Y, Ahmed Nadeem, Carberry Jaclyn, Teng Yue May Vannesa, Watkins Stuart, McComb Christie, Mangion Kenneth, McClure John D, Carrick David, O'Donnell Anna, Sood Arvind, McEntegart Margaret, Oldroyd Keith G, Radjenovic Aleksandra, Berry Colin
West of Scotland Heart and Lung Centre, Golden Jubilee National Hospital, Glasgow, United Kingdom.
BHF Glasgow Cardiovascular Research Centre, Institute of Cardiovascular and Medical Sciences, University of Glasgow, United Kingdom.
J Am Heart Assoc. 2017 Mar 31;6(4):e004759. doi: 10.1161/JAHA.116.004759.
Patients with recent non-ST-segment elevation myocardial infarction commonly have heterogeneous characteristics that may be challenging to assess clinically.
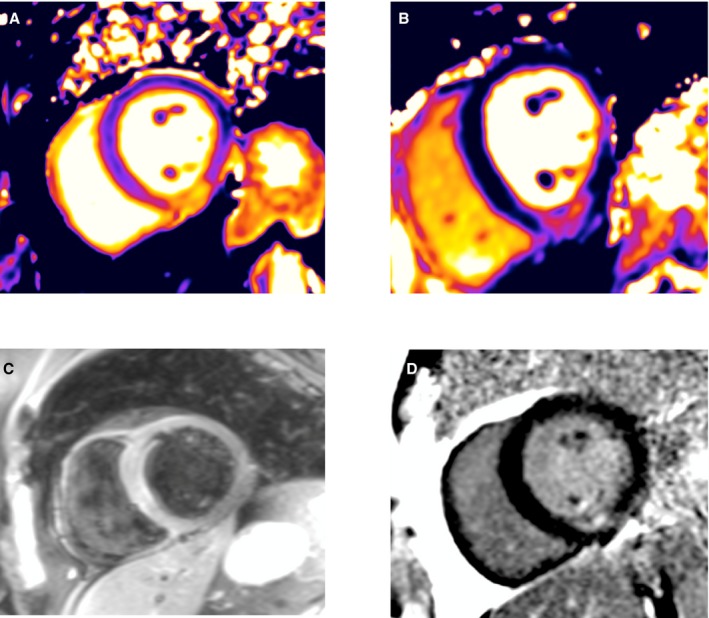
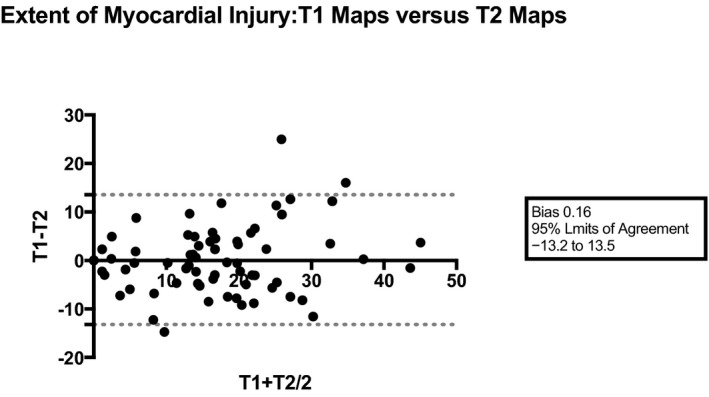
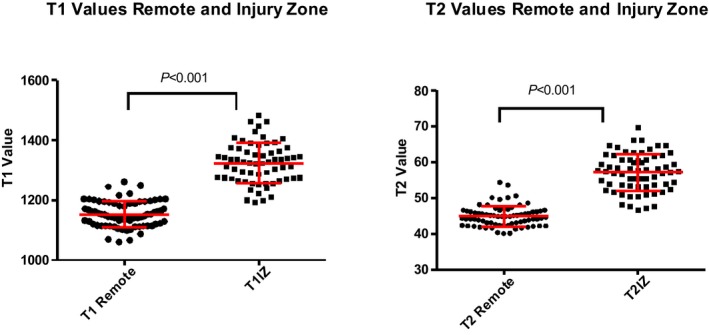
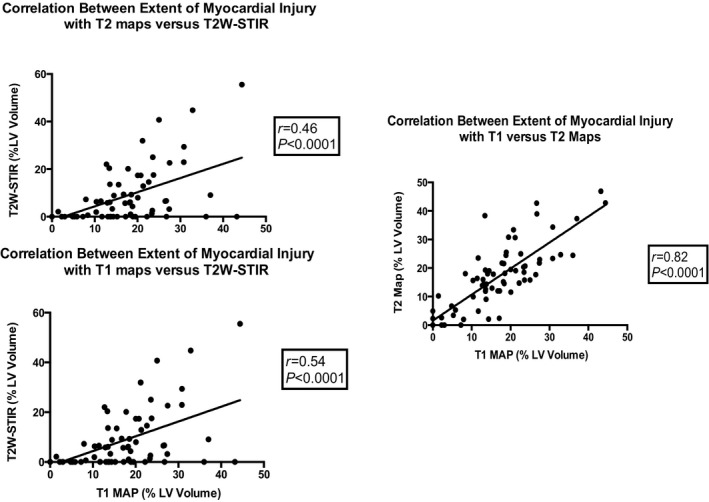
We prospectively studied the diagnostic accuracy of 2 novel (T1, T2 mapping) and 1 established (T2-weighted short tau inversion recovery [T2W-STIR]) magnetic resonance imaging methods for imaging the ischemic area at risk and myocardial salvage in 73 patients with non-ST-segment elevation myocardial infarction (mean age 57±10 years, 78% male) at 3.0-T magnetic resonance imaging within 6.5±3.5 days of invasive management. The infarct-related territory was identified independently using a combination of angiographic, ECG, and clinical findings. The presence and extent of infarction was assessed with late gadolinium enhancement imaging (gadobutrol, 0.1 mmol/kg). The extent of acutely injured myocardium was independently assessed with native T1, T2, and T2W-STIR methods. The mean infarct size was 5.9±8.0% of left ventricular mass. The infarct zone T1 and T2 times were 1323±68 and 57±5 ms, respectively. The diagnostic accuracies of T1 and T2 mapping for identification of the infarct-related artery were similar (=0.125), and both were superior to T2W-STIR (<0.001). The extent of myocardial injury (percentage of left ventricular volume) estimated with T1 (15.8±10.6%) and T2 maps (16.0±11.8%) was similar (=0.838) and moderately well correlated (=0.82, <0.001). Mean extent of acute injury estimated with T2W-STIR (7.8±11.6%) was lower than that estimated with T1 (<0.001) or T2 maps (<0.001).
In patients with non-ST-segment elevation myocardial infarction, T1 and T2 magnetic resonance imaging mapping have higher diagnostic performance than T2W-STIR for identifying the infarct-related artery. Compared with conventional STIR, T1 and T2 maps have superior value to inform diagnosis and revascularization planning in non-ST-segment elevation myocardial infarction.
URL: http://www.clinicaltrials.gov. Unique identifier: NCT02073422.
近期非ST段抬高型心肌梗死患者通常具有异质性特征,临床评估可能具有挑战性。
我们前瞻性研究了2种新型(T1、T2映射)和1种已确立的(T2加权短反转时间反转恢复序列[T2W-STIR])磁共振成像方法对73例非ST段抬高型心肌梗死患者(平均年龄57±10岁,78%为男性)在侵入性治疗后6.5±3.5天内于3.0-T磁共振成像上对危险缺血区域和心肌挽救情况进行成像的诊断准确性。通过血管造影、心电图和临床发现相结合的方法独立确定梗死相关区域。使用钆对比剂延迟强化成像(钆布醇,0.1 mmol/kg)评估梗死的存在和范围。使用T1、T2和T2W-STIR原始图像方法独立评估急性损伤心肌的范围。平均梗死面积为左心室质量的5.9±8.0%。梗死区域的T1和T2时间分别为1323±68和57±5毫秒。T1和T2映射识别梗死相关动脉的诊断准确性相似(=0.125),且均优于T2W-STIR(<0.001)。T1(15.8±10.6%)和T2映射(16.0±11.8%)估计的心肌损伤范围(左心室容积百分比)相似(= .838)且具有中度良好相关性(=0.82,<0.001)。T2W-STIR估计的急性损伤平均范围(7.8±11.6%)低于T1(<0.001)或T2映射(<0.001)。
在非ST段抬高型心肌梗死患者中,T1和T2磁共振成像映射在识别梗死相关动脉方面比T2W-STIR具有更高的诊断性能。与传统STIR相比,T1和T2映射在非ST段抬高型心肌梗死的诊断和血运重建规划方面具有更高的价值。