Stanton Michelle C, Yamauchi Masato, Mkwanda Square Z, Ndhlovu Paul, Matipula Dorothy Emmie, Mackenzie Charles, Kelly-Hope Louise A
Department of Parasitology, Liverpool School of Tropical Medicine, Liverpool, UK.
Ministry of Health, Lilongwe, Malawi.
Infect Dis Poverty. 2017 Apr 3;6(1):28. doi: 10.1186/s40249-017-0241-2.
Lymphatic filariasis (LF) is one of the primary causes of lymphoedema in sub-Saharan Africa, and has a significant impact on the quality of life (QoL) of those affected. In this paper we assess the relative impact of lymphoedema on mobility and income in Chikwawa district, Malawi.
A random sample of 31 people with lymphoedema and 31 matched controls completed a QoL questionnaire from which both an overall and a mobility-specific score were calculated. Two mobility tests were undertaken, namely the 10 m walking test [10MWT] and timed up and go [TUG] test, and a subset of 10 cases-control pairs wore GPS data loggers for 3 weeks to measure their mobility in a more natural setting. Retrospective economic data was collected from all 31 case-control pairs, and each participant undertaking the GPS activity recorded daily earnings and health expenditure throughout the observation period.
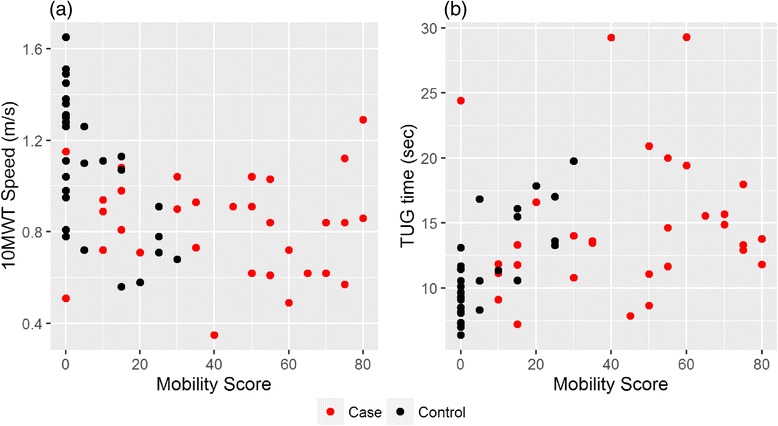
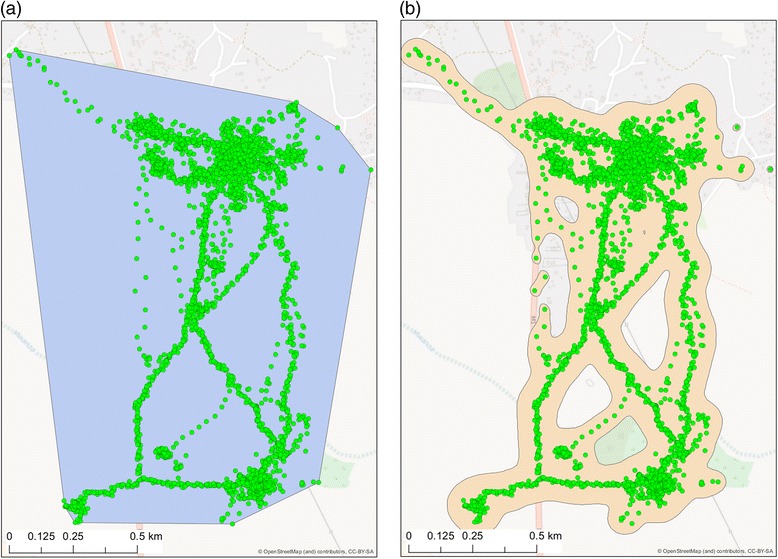
Cases had a significantly poorer overall QoL (cases = 32.2, controls = 6.0, P < 0.01) and mobility-specific (cases = 43.1, controls = 7.4, P < 0.01) scores in comparison to controls. Cases were also significantly slower (P < 0.01) at completing the timed mobility tests, e.g. mean 10MWT speed of 0.83 m/s in comparison to 1.10 m/s for controls. An inconsistent relationship was observed between mobility-specific QoL scores and the timed test results for cases (10MWT correlation = -0.06, 95% CI = (-0.41, 0.30)), indicating that their perceived disability differed from their measured disability, whereas the results were consistent for controls (10MWT correlation = -0.61, 95% CI = (-0.79, -0.34)). GPS summaries indicated that cases generally walk shorter distances at slower speeds than control, covering a smaller geographical area (median area by kernel smoothing: cases = 1.25 km, controls = 2.10 km, P = 0.16). Cases reported earning less than half that earned by controls per week (cases = $0.70, controls = $1.86, P = 0.064), with a smaller proportion of their earnings (16% vs 22%, P = 0.461) being spent on healthcare.
Those affected by lymphoedema are at a clear disadvantage to their unaffected peers, experiencing a lower QoL as confirmed by both subjective and objective mobility measures, and lower income. This study also indicates that objective measures of mobility may be a useful supplement to self-assessed QoL questionnaires when assessing the future impact of lymphoedema management interventions.
淋巴丝虫病(LF)是撒哈拉以南非洲淋巴水肿的主要病因之一,对患者的生活质量(QoL)有重大影响。本文评估了马拉维奇夸瓦区淋巴水肿对行动能力和收入的相对影响。
随机抽取31名淋巴水肿患者和31名匹配的对照完成一份生活质量问卷,计算出总体得分和特定行动能力得分。进行了两项行动能力测试,即10米步行测试[10MWT]和计时起立行走测试[TUG],10对病例-对照对子佩戴GPS数据记录器3周,以测量他们在更自然环境中的行动能力。从所有31对病例-对照对子中收集回顾性经济数据,参与GPS活动的每位参与者记录观察期内的每日收入和医疗支出。
与对照组相比,病例的总体生活质量得分(病例=32.2,对照=6.0,P<0.01)和特定行动能力得分(病例=43.1,对照=7.4,P<0.01)明显更低。病例在完成计时行动能力测试时也明显更慢(P<0.01),例如10MWT的平均速度为0.83米/秒,而对照组为1.10米/秒。病例特定行动能力生活质量得分与计时测试结果之间存在不一致的关系(10MWT相关性=-0.06,95%CI=(-0.41,0.30)),表明他们感知到的残疾与测量到的残疾不同,而对照组的结果是一致的(10MWT相关性=-0.61,95%CI=(-0.79,-0.34))。GPS总结表明,病例通常行走距离更短、速度更慢,覆盖的地理区域更小(核密度估计的中位数面积:病例=1.25千米,对照=2.10千米,P=0.16)。病例报告每周收入不到对照组的一半(病例=0.70美元,对照=1.86美元,P=0.064),他们用于医疗保健的收入比例更小(16%对22%,P=0.461)。
淋巴水肿患者与其未受影响的同龄人相比明显处于劣势,主观和客观行动能力测量均证实其生活质量较低,收入也较低。本研究还表明,在评估淋巴水肿管理干预措施的未来影响时,行动能力的客观测量可能是自我评估生活质量问卷的有用补充。