Choudhary Richa, Sitaraman Sadasivan, Choudhary Anita
Department of Pediatrics, Sawai Man Singh Medical College, Sir Padampat Mother and Child Health Institute, Jaipur, Rajasthan, India.
J Emerg Trauma Shock. 2017 Apr-Jun;10(2):55-59. doi: 10.4103/JETS.JETS_103_16.
Septic shock can rapidly evolve into multiple system organ failure and death. In the recent years, hyperlactatemia has been found to be a risk factor for mortality in critically ill adults.
To evaluate the predictive value of lactate clearance and to determine the optimal cut-off value for predicting outcome in children with septic shock.
A prospective observational study was performed on children with septic shock admitted to pediatric Intensive Care Unit (PICU).
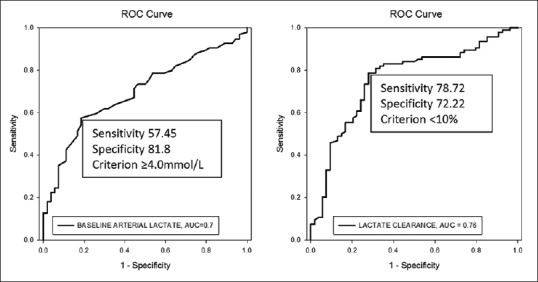
Serial lactate levels were measured at PICU admission, 24 and 48 h later. Lactate clearance, percent decrease in lactate level in 24 h, was calculated. The primary outcome measure was survival or nonsurvival at the end of hospital stay. We performed receiver operating characteristic analyses to calculate optimal cut-off values.
The mean lactate levels at admission were significantly higher in the nonsurvivors than survivors, 5.12 ± 3.51 versus 3.13 ± 1.71 mmol/L ( = 0.0001). The cut-off for lactate level at admission for the best prediction of mortality was determined as ≥4 mmol/L (odds ratio 5.4; 95% confidence interval [CI] =2.45-12.09). Mean lactate clearance was significantly higher in survivors than nonsurvivors (17.9 ± 39.9 vs. -23.2 ± 62.7; < 0.0001). A lactate clearance rate of <10% at 24 h had a sensitivity and specificity of 78.7% and 72.2%, respectively and a positive predictive value of 83.1% for death. Failure to achieve a lactate clearance of more than 10% was associated with greater risk of mortality (likelihood ratio + 2.83; 95% CI = 1.82-4.41).
Serial lactate levels can be used to predict outcome in pediatric septic shock. A 24 h lactate clearance cut-off of <10% is a predictor of in-hospital mortality in such patients.
感染性休克可迅速发展为多系统器官功能衰竭并导致死亡。近年来,高乳酸血症已被发现是危重症成年患者死亡的一个危险因素。
评估乳酸清除率的预测价值,并确定预测感染性休克患儿预后的最佳临界值。
对入住儿科重症监护病房(PICU)的感染性休克患儿进行了一项前瞻性观察研究。
在患儿入住PICU时、24小时及48小时后分别测量系列乳酸水平。计算乳酸清除率,即24小时内乳酸水平下降的百分比。主要结局指标是住院期末的存活或死亡情况。我们进行了受试者工作特征分析以计算最佳临界值。
非存活者入院时的平均乳酸水平显著高于存活者,分别为5.12±3.51 mmol/L和3.13±1.71 mmol/L(P = 0.0001)。确定入院时乳酸水平对死亡率进行最佳预测的临界值为≥4 mmol/L(比值比5.4;95%置信区间[CI]=2.45 - 12.09)。存活者的平均乳酸清除率显著高于非存活者(17.9±39.9对 - 23.2±62.7;P < 0.0001)。24小时时乳酸清除率<10%的敏感度和特异度分别为78.7%和72.2%,死亡的阳性预测值为83.1%。未能实现超过10%的乳酸清除率与更高的死亡风险相关(似然比+2.83;95% CI = 1.82 - 4.41)。
系列乳酸水平可用于预测儿科感染性休克的预后。24小时乳酸清除率<10%是此类患者院内死亡率的一个预测指标。