Gurel Michelle H, Han Yi, Stevens Andrea L, Furtado Aaron, Cox David
Neuroendocrine and Pituitary Tumor Clinical Center, Massachusetts General Hospital, Zero Emerson Place, Suite 112, Boston, MA, 02114, USA.
WG Consulting, 200 Fifth Ave, New York, NY, 10010, USA.
BMC Pharmacol Toxicol. 2017 Apr 4;18(1):22. doi: 10.1186/s40360-017-0124-y.
Many patients with acromegaly require medical treatment that includes somatostatin analogs (SSAs). Long-acting SSA formulations are widely used, due in part to increased patient convenience and increased treatment adherence vs daily medications. Although medication compliance can be poor in patients with chronic conditions, adherence and persistence with these SSAs in patients with acromegaly has not been evaluated. This analysis utilized claims data to estimate treatment adherence and persistence for lanreotide depot and long-acting octreotide in this population.
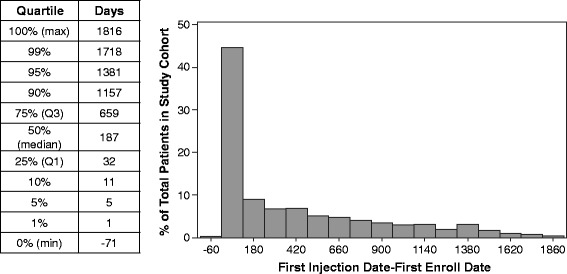
This retrospective analysis used the MarketScan® database (~100 payors, 500 million claims in the US), which was searched between January 2007 and June 2012 to identify patients with acromegaly taking either lanreotide depot or long-acting octreotide. Patients switching treatments were excluded. Treatment adherence was assessed using medication possession ratio (MPR; number of doses dispensed in relation to dispensing period; ≥80% is considered adherent), injection count, and treatment time. Persistence was estimated by Kaplan-Meier analyses and Cox proportional hazards modeling. A washout period, defined as no acromegaly-related prescription activity 180 days prior to the index date, was employed to minimize effects of prior therapy and focus on patients more likely to be treatment-naïve.
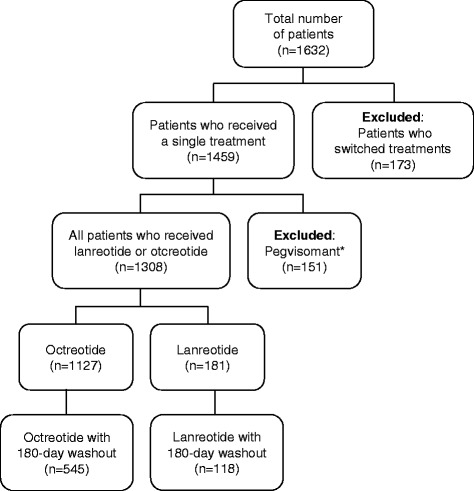
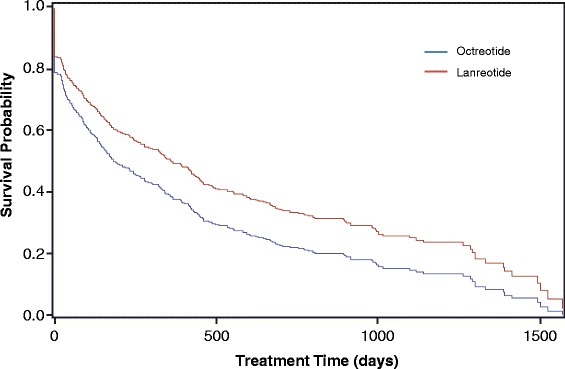
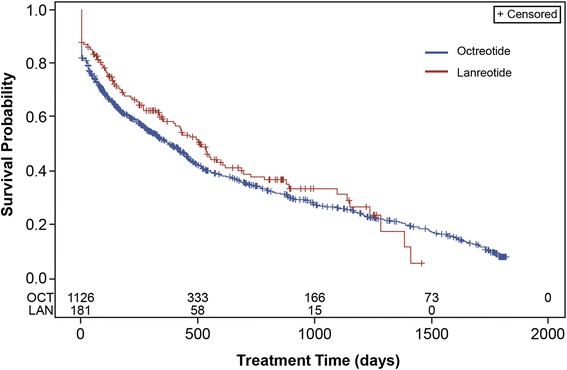
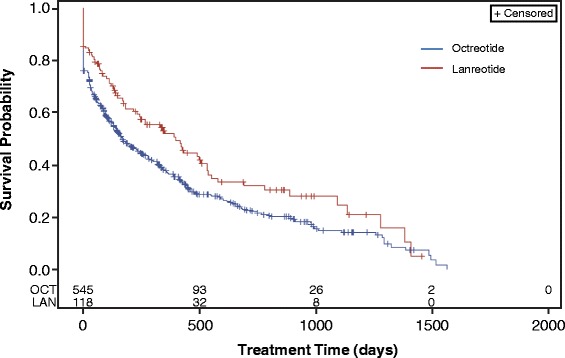
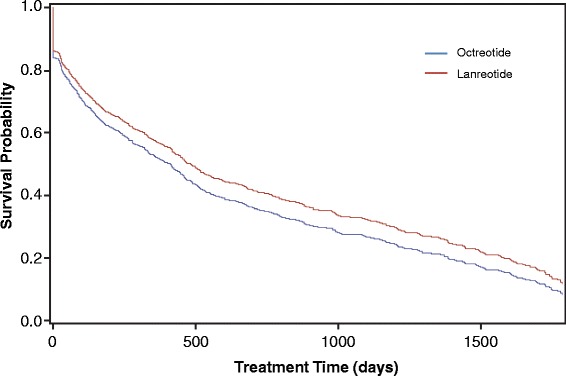
Altogether 1308 patients with acromegaly receiving a single SSA for treatment (1127 octreotide, 181 lanreotide) who had not switched treatments were identified. Mean MPR in patients with a 180-day washout (n = 663) was 89% for those receiving octreotide (n = 545) and 87% for those receiving lanreotide (n = 118). Median number of days on therapy was 169 (95% CI 135-232) for octreotide patients and 400 (95% CI 232-532) for lanreotide patients. The point estimate of the Cox proportional hazard ratio for stopping treatment was 1.385 for octreotide vs lanreotide (95% CI 1.079-1.777), suggesting a 38.5% increased risk for stopping octreotide before lanreotide.
Treatment adherence was similarly good for both injectable SSA treatments studied, at 87% or greater. Persistence was greater with lanreotide than octreotide and the risk of discontinuing therapy was lower with lanreotide than octreotide. Further studies to determine factors leading to these differences in persistence or to predict discontinuation of therapy may aid in clinical management of these patients.
许多肢端肥大症患者需要包括生长抑素类似物(SSA)在内的药物治疗。长效SSA制剂被广泛使用,部分原因是相较于每日用药,它提高了患者的便利性并增强了治疗依从性。尽管慢性病患者的药物依从性可能较差,但肢端肥大症患者对这些SSA的依从性和持续性尚未得到评估。本分析利用索赔数据来估计该人群中长效兰瑞肽和长效奥曲肽的治疗依从性和持续性。
这项回顾性分析使用了MarketScan®数据库(美国约100个付款方,5亿条索赔记录),在2007年1月至2012年6月期间进行检索,以识别正在服用长效兰瑞肽或长效奥曲肽的肢端肥大症患者。排除了更换治疗方案的患者。使用药物持有率(MPR;配药剂量与配药期的关系;≥80%被视为依从)、注射次数和治疗时间来评估治疗依从性。通过Kaplan-Meier分析和Cox比例风险模型估计持续性。采用洗脱期,定义为索引日期前180天内无肢端肥大症相关处方活动,以尽量减少先前治疗的影响,并关注更可能未接受过治疗的患者。
共识别出1308例未更换治疗方案且接受单一SSA治疗的肢端肥大症患者(1127例接受奥曲肽,181例接受兰瑞肽)。有180天洗脱期的患者(n = 663)中,接受奥曲肽治疗的患者(n = 545)的平均MPR为89%,接受兰瑞肽治疗的患者(n = 118)为87%。奥曲肽患者的中位治疗天数为169天(95%CI 135 - 232),兰瑞肽患者为400天(95%CI 232 - 532)。奥曲肽与兰瑞肽相比,停止治疗的Cox比例风险比的点估计值为1.385(95%CI 1.079 - 1.777),表明在兰瑞肽之前停止使用奥曲肽的风险增加38.