Asfalou Iliyasse, Boulaamayl Sanae, Raissouni Maha, Mouine Najat, Sabry Mohamed, Kheyi Jamal, Doghmi Nawal, Benyass Aatif
Department of Cardiac Non-Invasive Explorations, Mohamed V Military Hospital, IBN SINA Hospital Center, Mohamed V University, Rabat, aMorocco.
Department of Cardiology B, IBN SINA Hospital Center, Mohamed V University, Rabat, bMorocco.
J Saudi Heart Assoc. 2017 Apr;29(2):102-109. doi: 10.1016/j.jsha.2016.02.004. Epub 2016 Mar 11.
To describe modes of clinical presentation and echocardiographic, angiographic, and rhythmic features, and prognostic characteristics of left ventricular noncompaction cardiomyopathy (LVNC) in North African adults, through one of the first series in Morocco.
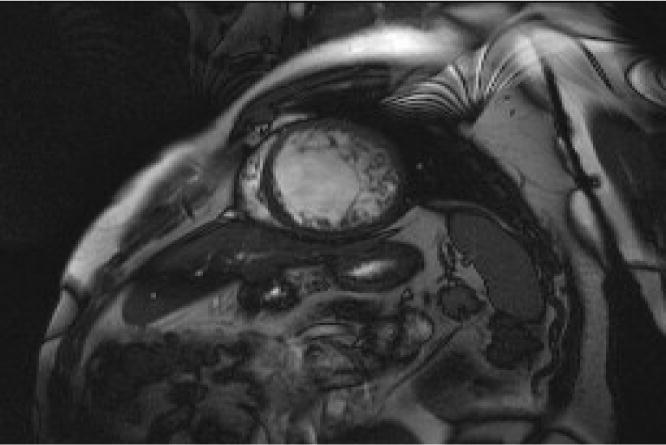
LVNC is a rare congenital disorder, described for the first time by Engberding in 1984. The suspected diagnosis in thromboembolic, hemodynamic, or rhythm events requires both echocardiography and cardiovascular magnetic resonance (CMR). Its therapeutic management is not yet well codified but akin to that proposed for dilated cardiomyopathy.
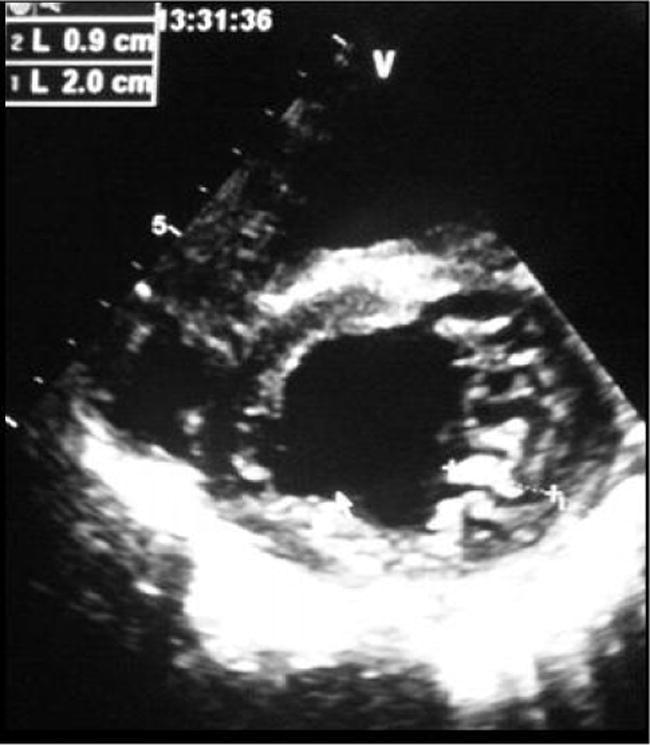
This study included a retrospective, descriptive, and analytical cohort of 23 cases of cardiomyopathy with LVNC diagnosed in the Noninvasive Explorations Laboratory at the Military Hospital of Rabat, Morocco, between January 2009 and October 2014. The echocardiographic criteria for LVNC include the absence of any coexisting cardiac anomalies. The characteristic appearance of numerous excessively prominent trabeculations and deep intertrabecular recesses and intertrabecular spaces filled by direct blood flow from the ventricular cavity, as visualized on color Doppler imaging with noncompacted/compacted ratio > 2 according to Jenni criteria. Twenty-three adults fulfilled the diagnostic criteria and were followed prospectively.
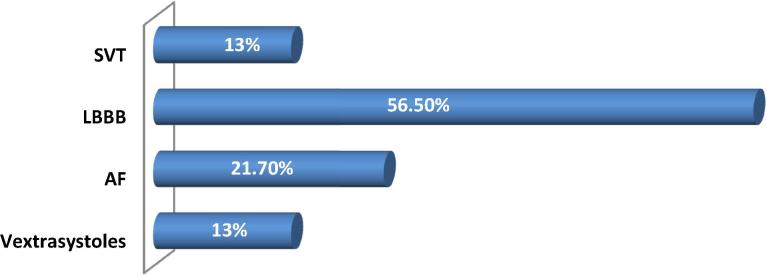
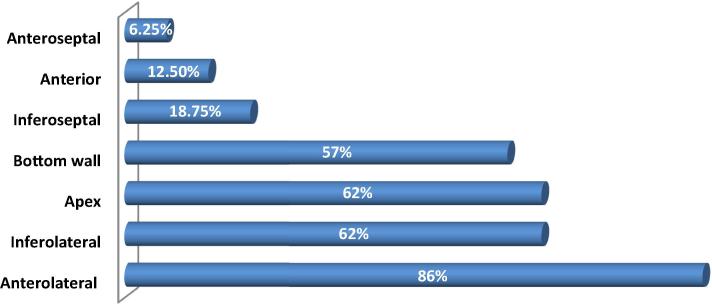
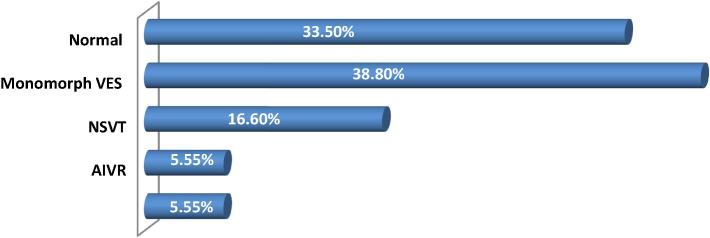
At diagnosis, the mean age was 47 ± 13 years with a male predominance at 65.2%. Of them, 56.5% had a left bundle branch block and 21.7% were in atrial fibrillation. Left ventricular end-diastolic diameter was 67.7 ± 6.6 mm and ejection fraction was at 27 ± 8%. Apex and/or midventricular segments of both the inferior and lateral wall were involved in more than 80% of patients with an average of 4.8 noncompacted segments. CMR was performed in 12 patients and was decisive for the diagnosis. Major complications were heart failure in 31% of patients, ventricular tachycardia in three patients, and thromboembolic events in one patient. Twenty eight point six percent of patients started a long-term anticoagulant therapy. One patient underwent implantation of a double-room pacemaker. Automated defibrillators were implanted in two patients. There were three deaths: one sudden death and two end-stage heart failure.
LVNC should be looked for at any dilated cardiomyopathy particularly in young patients. It requires a careful echocardiographic examination and sometimes CMR to confirm the diagnosis. It is characterized by severe systolic and diastolic dysfunction that would provide poor prognosis.
通过摩洛哥首批系列研究之一,描述北非成年人左心室心肌致密化不全(LVNC)的临床表现模式、超声心动图、血管造影和节律特征以及预后特点。
LVNC是一种罕见的先天性疾病,1984年由Engberding首次描述。对于血栓栓塞、血流动力学或节律事件的疑似诊断需要超声心动图和心血管磁共振(CMR)检查。其治疗管理尚未得到很好的规范,但类似于扩张型心肌病的治疗方案。
本研究纳入了2009年1月至2014年10月在摩洛哥拉巴特军事医院无创检查实验室诊断为LVNC的23例心肌病患者的回顾性、描述性和分析性队列。LVNC的超声心动图标准包括不存在任何并存的心脏异常。根据Jenni标准,在彩色多普勒成像上可见大量过度突出的小梁、深陷的小梁间隐窝以及由心室腔直接血流填充的小梁间间隙,非致密化/致密化比率>2,即为其特征性表现。23名成年人符合诊断标准并进行了前瞻性随访。
诊断时,平均年龄为47±13岁,男性占65.2%。其中,56.5%有左束支传导阻滞,21.7%为心房颤动。左心室舒张末期内径为67.7±6.6mm,射血分数为27±8%。下壁和侧壁的心尖和/或心室中段节段受累超过80%的患者,平均有4.8个非致密化节段。12名患者进行了CMR检查,对诊断起决定性作用。主要并发症包括31%的患者发生心力衰竭,3名患者发生室性心动过速,1名患者发生血栓栓塞事件。28.6%的患者开始接受长期抗凝治疗。1名患者植入了双腔起搏器。2名患者植入了自动除颤器。有3例死亡:1例猝死,2例终末期心力衰竭。
对于任何扩张型心肌病,尤其是年轻患者,都应考虑LVNC。确诊需要仔细的超声心动图检查,有时还需要CMR检查。其特征为严重的收缩和舒张功能障碍,预后较差。