Griffiths James, Carnegie Amadeus, Kendall Richard, Madan Rajeev
School of Clinical Medicine, University of Cambridge, Cambridge, UK.
Robinson College, Grange Road, Cambridge, CB3 9AN, UK.
Crit Ultrasound J. 2017 Dec;9(1):9. doi: 10.1186/s13089-017-0064-1. Epub 2017 Apr 3.
Ultrasound-guided peripheral intravenous access may present an alternative to central or intraosseous access in patients with difficult peripheral veins. Using venepuncture of a phantom model as a proxy, we investigated whether novice ultrasound users should adopt a cross-sectional or longitudinal approach when learning to access peripheral veins under ultrasound guidance. This result would inform the development of a structured training method for this procedure.
We conducted a randomised controlled trial of 30 medical students. Subjects received 35 min of training, then attempted to aspirate 1 ml of synthetic blood from a deep vein in a training model under ultrasound guidance. Subjects attempted both the cross-sectional and longitudinal approaches. Group 1 used cross-sectional first, followed by longitudinal. Group 2 used longitudinal first, then cross-sectional. We measured the time from first puncture of the model's skin to aspiration of fluid, and the number of attempts required. Subjects also reported difficulty ratings for each approach. Paired sample t-tests were used for statistical analysis.
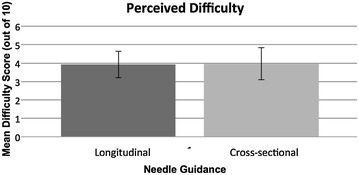
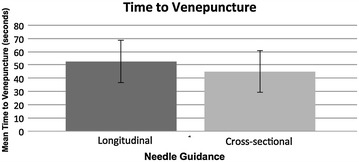
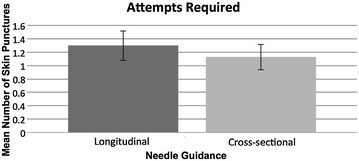
The mean number of attempts was 1.13 using the cross-sectional approach, compared with 1.30 using the longitudinal approach (p = 0.17). Mean time to aspiration of fluid was 45.1 s using the cross-sectional approach and 52.8 s using the longitudinal approach (p = 0.43). The mean difficulty score out of 10 was 3.97 for the cross-sectional approach and 3.93 for the longitudinal approach (p = 0.95).
We found no significant difference in effectiveness between the cross-sectional and longitudinal approaches to ultrasound-guided venepuncture when performed on a model. We believe that both approaches should be included when teaching ultrasound-guided peripheral vascular access. To confirm which approach would be best in clinical practice, we advocate future testing of both approaches on patients.
对于外周静脉条件较差的患者,超声引导下的外周静脉穿刺可能是中心静脉或骨内通路的一种替代方法。我们以模拟模型的静脉穿刺作为替代,研究了新手超声使用者在学习超声引导下外周静脉穿刺时应采用横断面法还是纵断面法。该结果将为该操作的结构化培训方法的开发提供参考。
我们对30名医学生进行了一项随机对照试验。受试者接受35分钟的培训,然后在超声引导下尝试从训练模型的深静脉中抽取1毫升模拟血液。受试者分别尝试横断面法和纵断面法。第一组先采用横断面法,然后采用纵断面法。第二组先采用纵断面法,然后采用横断面法。我们测量了从首次穿刺模型皮肤到抽出液体的时间以及所需的尝试次数。受试者还报告了每种方法的难度等级。采用配对样本t检验进行统计分析。
采用横断面法时平均尝试次数为1.13次,而采用纵断面法时为1.30次(p = 0.17)。采用横断面法时抽出液体的平均时间为45.1秒,采用纵断面法时为52.8秒(p = 0.43)。横断面法的平均难度评分为3.97分(满分10分),纵断面法为3.93分(p = 0.95)。
我们发现在模型上进行超声引导静脉穿刺时,横断面法和纵断面法在有效性上无显著差异。我们认为在教授超声引导外周血管穿刺时应同时包含这两种方法。为确定哪种方法在临床实践中最佳,我们主张未来在患者身上对这两种方法进行测试。