Kristen Arnt V, Maurer Mathew S, Rapezzi Claudio, Mundayat Rajiv, Suhr Ole B, Damy Thibaud
Amyloidosis Center, Department of Cardiology, Heidelberg University, Heidelberg, Germany.
Center for Advanced Cardiac Care, Columbia University Medical Center, New York, New York, United States of America.
PLoS One. 2017 Apr 6;12(4):e0173086. doi: 10.1371/journal.pone.0173086. eCollection 2017.
Cardiac troponins and natriuretic peptides are established for risk stratification in light-chain amyloidosis. Data on cardiac biomarkers in transthyretin amyloidosis (ATTR) are lacking.
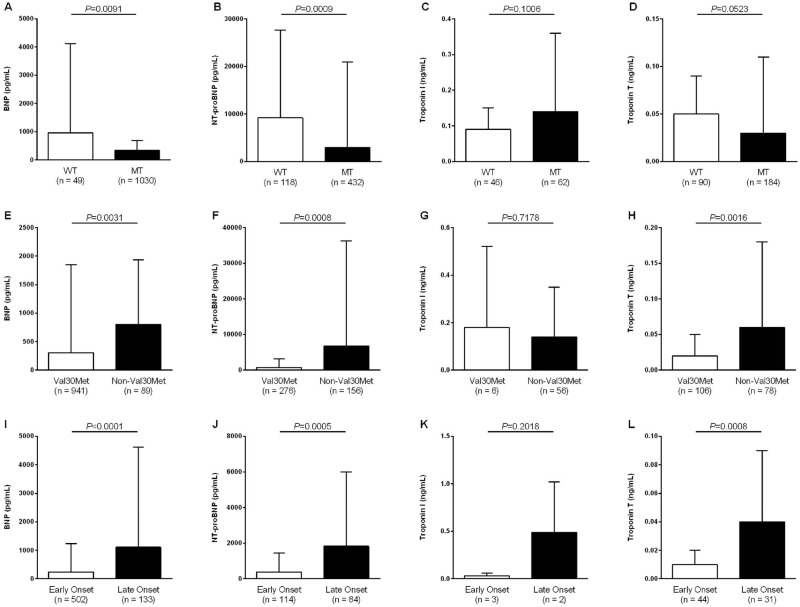
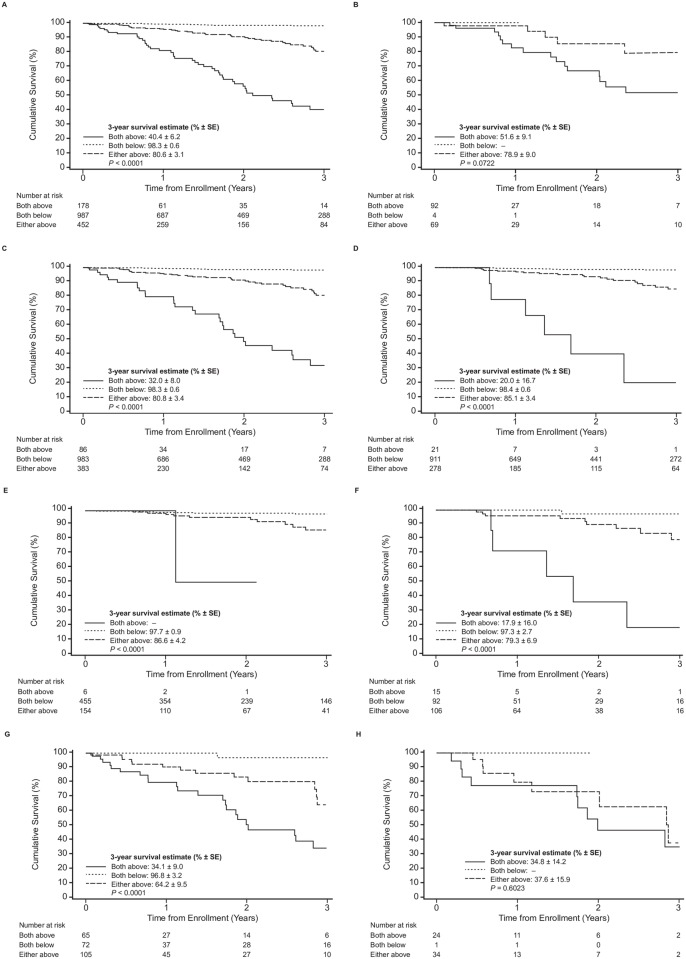
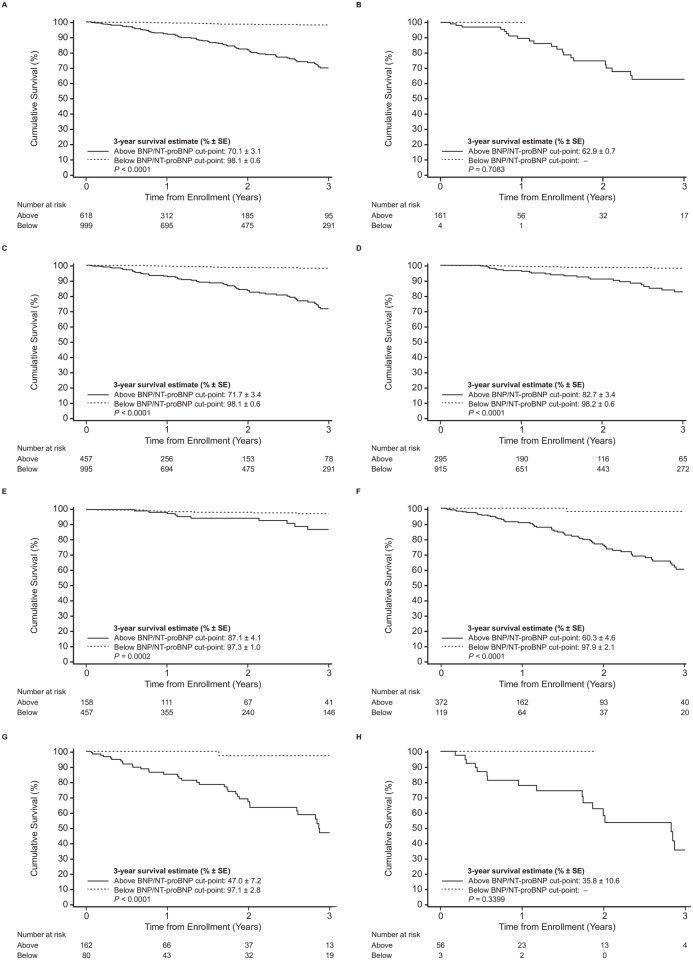
Patients (n = 1617) with any of the following cardiac biomarkers, BNP (n = 1079), NT-proBNP (n = 550), troponin T (n = 274), and troponin I (n = 108), available at baseline in the Transthyretin Amyloidosis Outcomes Survey (THAOS) were analyzed for differences between genotypes and phenotypes and their association with survival. Median level of BNP was 68.0 pg/mL (IQR 30.5-194.9), NT-proBNP 337.9 pg/mL (IQR 73.0-2584.0), troponin T 0.03 μg/L (IQR 0.01-0.05), and troponin I 0.08 μg/L (IQR 0.04-0.13). NT-proBNP and BNP were higher in wild-type than mutant-type ATTR, troponin T and I did not differ, respectively. Non-Val30Met patients had higher BNP, NT-proBNP and troponin T levels than Val30Met patients, but not troponin I. Late-onset Val30Met was associated with higher levels of troponin I and troponin T compared with early-onset. 115 patients died during a median follow-up of 1.2 years. Mortality increased with increasing quartiles (BNP/NT-proBNP Q1 = 1.7%, Q2 = 5.2%, Q3 = 21.7%, Q4 = 71.3%; troponin T/I Q1 = 6.5%, Q2 = 14.5%, Q3 = 33.9%, Q4 = 45.2%). Three-year overall-survival estimates for BNP/NT-proBNP and troponin T/I quartiles differed significantly (p<0.001). Stepwise risk stratification was achieved by combining NT-proBNP/BNP and troponin T/I. From Cox proportional hazards model, age, modified body mass index, mutation (Val30Met vs. Non-Val30Met) and BNP/NT-proBNP (Q1-Q3 pooled vs. Q4) were identified as independent predictors of survival in patients with mutant-type ATTR.
In this ATTR patient cohort, cardiac biomarkers were abnormal in a substantial percentage of patients irrespective of genotype. Along with age, mBMI, and mutation (Val30Met vs. Non-Val30Met), cardiac biomarkers were associated with surrogates of disease severity with BNP/NT-proBNP identified as an independent predictor of survival in ATTR.
ClinicalTrials.gov NCT00628745.
心肌肌钙蛋白和利钠肽已被用于轻链淀粉样变性的危险分层。关于转甲状腺素蛋白淀粉样变性(ATTR)中心脏生物标志物的数据尚缺乏。
在转甲状腺素蛋白淀粉样变性结局调查(THAOS)中,分析了1617例患者,这些患者在基线时具有以下任何一种心脏生物标志物:脑钠肽(BNP,n = 1079)、N末端脑钠肽前体(NT-proBNP,n = 550)、肌钙蛋白T(n = 274)和肌钙蛋白I(n = 108),以比较基因型和表型之间的差异及其与生存的关系。BNP的中位数水平为68.0 pg/mL(四分位间距30.5 - 194.9),NT-proBNP为337.9 pg/mL(四分位间距73.0 - 2584.0),肌钙蛋白T为0.03 μg/L(四分位间距0.01 - 0.05),肌钙蛋白I为0.08 μg/L(四分位间距0.04 - 0.13)。野生型ATTR患者的NT-proBNP和BNP高于突变型,肌钙蛋白T和肌钙蛋白I则无差异。非Val30Met患者的BNP、NT-proBNP和肌钙蛋白T水平高于Val30Met患者,但肌钙蛋白I无差异。与早发型相比,晚发型Val30Met与更高水平肌钙蛋白I和肌钙蛋白T相关。在中位随访1.2年期间,115例患者死亡。死亡率随四分位数增加而升高(BNP/NT-proBNP:第一四分位数 = 1.7%,第二四分位数 = 5.2%,第三四分位数 = 21.7%,第四四分位数 = 71.3%;肌钙蛋白T/I:第一四分位数 = 6.5%,第二四分位数 = 14.5%,第三四分位数 = 33.9%,第四四分位数 = 45.2%)。BNP/NT-proBNP和肌钙蛋白T/I四分位数的三年总生存率估计值有显著差异(p<0.001)。通过结合NT-proBNP/BNP和肌钙蛋白T/I实现逐步危险分层。从Cox比例风险模型中,年龄、改良体重指数、突变(Val30Met与非Val30Met)以及BNP/NT-proBNP(第一至第三四分位数合并与第四四分位数)被确定为突变型ATTR患者生存的独立预测因素。
在这个ATTR患者队列中,无论基因型如何,相当比例患者的心脏生物标志物异常。除年龄、改良体重指数和突变(Val30Met与非Val30Met)外,心脏生物标志物与疾病严重程度指标相关,BNP/NT-proBNP被确定为ATTR患者生存的独立预测因素。
ClinicalTrials.gov NCT00628745