Hendriks Tom, Hartman Minke H T, Vlaar Pieter J J, Prakken Niek H J, van der Ende Yldau M Y, Lexis Chris P H, van Veldhuisen Dirk J, van der Horst Iwan C C, Lipsic Erik, Nijveldt Robin, van der Harst Pim
Department of Cardiology, University of Groningen, University Medical Center Groningen, Hanzeplein 1, 9700 RB, Groningen, The Netherlands.
Department of Radiology, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands.
Int J Cardiovasc Imaging. 2017 Sep;33(9):1415-1423. doi: 10.1007/s10554-017-1131-1. Epub 2017 Apr 7.
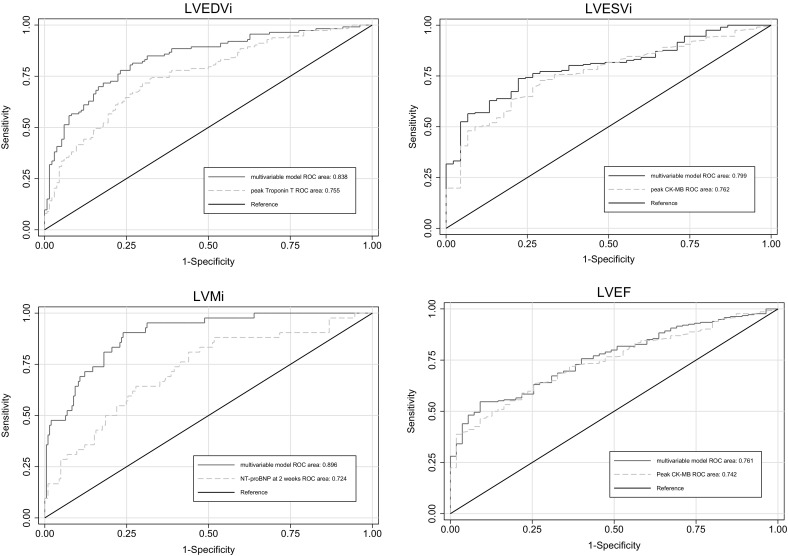
Adverse left ventricular (LV) remodeling after acute ST-elevation myocardial infarction (STEMI) is associated with morbidity and mortality. We studied clinical, biochemical and angiographic determinants of LV end diastolic volume index (LVEDVi), end systolic volume index (LVESVi) and mass index (LVMi) as global LV remodeling parameters 4 months after STEMI, as well as end diastolic wall thickness (EDWT) and end systolic wall thickness (ESWT) of the non-infarcted myocardium, as compensatory remote LV remodeling parameters. Data was collected in 271 patients participating in the GIPS-III trial, presenting with a first STEMI. Laboratory measures were collected at baseline, 2 weeks, and 6-8 weeks. Cardiovascular magnetic resonance imaging (CMR) was performed 4 months after STEMI. Linear regression analyses were performed to determine predictors. At baseline, patients were 21% female, median age was 58 years. At 4 months, mean LV ejection fraction (LVEF) was 54 ± 9%, mean infarct size was 9.0 ± 7.9% of LVM. Strongest univariate predictors (all p < 0.001) were peak Troponin T for LVEDVi (R = 0.26), peak CK-MB for LVESVi (R = 0.41), NT-proBNP at 2 weeks for LVMi (R = 0.24), body surface area for EDWT (R = 0.32), and weight for ESWT (R = 0.29). After multivariable analysis, cardiac biomarkers remained the strongest predictors of LVMi, LVEDVi and LVESVi. NT-proBNP but none of the acute cardiac injury biomarkers were associated with remote LV wall thickness. Our analyses illustrate the value of cardiac specific biochemical biomarkers in predicting global LV remodeling after STEMI. We found no evidence for a hypertrophic response of the non-infarcted myocardium.
急性ST段抬高型心肌梗死(STEMI)后左心室(LV)不良重构与发病率和死亡率相关。我们研究了STEMI后4个月时左心室舒张末期容积指数(LVEDVi)、收缩末期容积指数(LVESVi)和质量指数(LVMi)作为整体左心室重构参数的临床、生化和血管造影决定因素,以及非梗死心肌的舒张末期壁厚(EDWT)和收缩末期壁厚(ESWT)作为代偿性远隔左心室重构参数。收集了参与GIPS-III试验的271例首次发生STEMI患者的数据。在基线、2周和6 - 8周时收集实验室指标。在STEMI后4个月进行心血管磁共振成像(CMR)检查。进行线性回归分析以确定预测因素。基线时,患者中女性占21%,中位年龄为58岁。4个月时,平均左心室射血分数(LVEF)为54±9%,平均梗死面积为左心室心肌质量的9.0±7.9%。最强的单变量预测因素(均p<0.001)为:LVEDVi的肌钙蛋白T峰值(R = 0.26)、LVESVi的肌酸激酶同工酶MB峰值(R = 0.41)、2周时的NT-proBNP用于LVMi(R = 0.24)、体表面积用于EDWT(R = 0.32)以及体重用于ESWT(R = 0.29)。多变量分析后,心脏生物标志物仍然是LVMi、LVEDVi和LVESVi的最强预测因素。NT-proBNP,但急性心脏损伤生物标志物均与远隔左心室壁厚度无关。我们的分析说明了心脏特异性生化生物标志物在预测STEMI后整体左心室重构中的价值。我们未发现非梗死心肌肥厚反应的证据。