Dranitsaris G, Molassiotis A, Clemons M, Roeland E, Schwartzberg L, Dielenseger P, Jordan K, Young A, Aapro M
The Ottawa Hospital Regional Cancer Centre, Ottawa, Canada.
Hong Kong Polytechnic University, Hong Kong.
Ann Oncol. 2017 Jun 1;28(6):1260-1267. doi: 10.1093/annonc/mdx100.
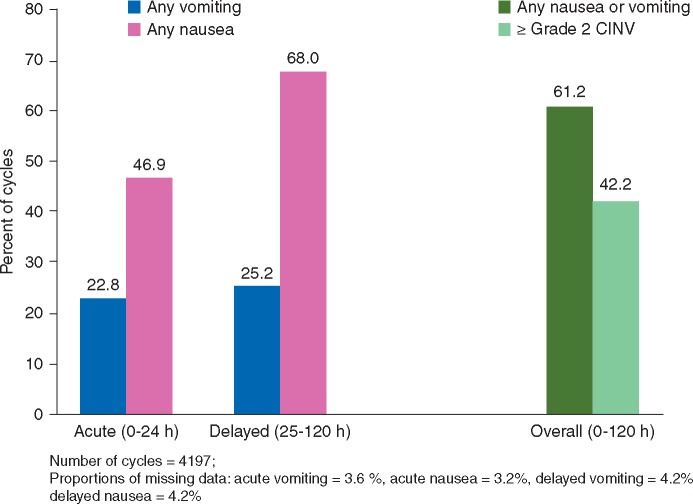
Despite the availability of effective antiemetics and evidence-based guidelines, up to 40% of cancer patients receiving chemotherapy fail to achieve complete nausea and vomiting control. In addition to type of chemotherapy, several patient-related risk factors for chemotherapy-induced nausea and vomiting (CINV) have been identified. To incorporate these factors into the optimal selection of prophylactic antiemetics, a repeated measures cycle-based model to predict the risk of ≥ grade 2 CINV (≥2 vomiting episodes or a decrease in oral intake due to nausea) from days 0 to 5 post-chemotherapy was developed.
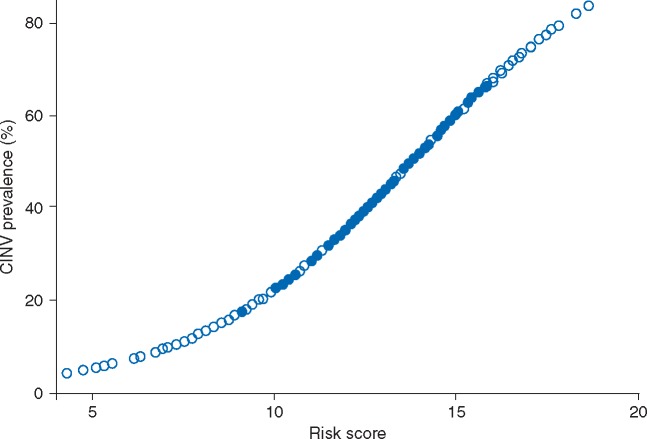
Data from 1198 patients enrolled in one of the five non-interventional CINV prospective studies were pooled. Generalized estimating equations were used in a backwards elimination process with the P-value set at <0.05 to identify the relevant predictive factors. A risk scoring algorithm (range 0-32) was then derived from the final model coefficients. Finally, a receiver-operating characteristic curve (ROCC) analysis was done to measure the predictive accuracy of the scoring algorithm.
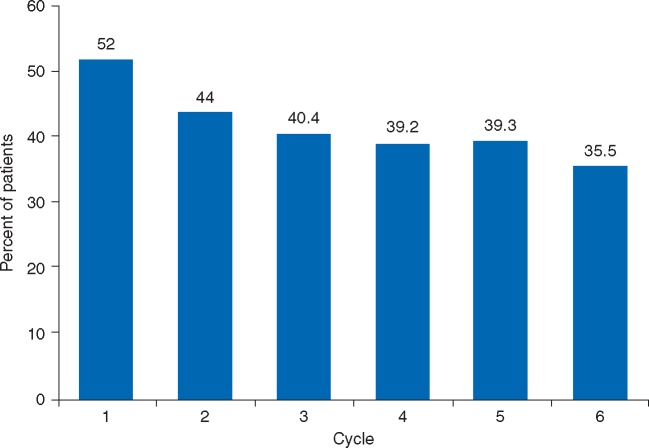
Over 4197 chemotherapy cycles, 42.2% of patients experienced ≥grade 2 CINV. Eight risk factors were identified: patient age <60 years, the first two cycles of chemotherapy, anticipatory nausea and vomiting, history of morning sickness, hours of sleep the night before chemotherapy, CINV in the prior cycle, patient self-medication with non-prescribed treatments, and the use of platinum or anthracycline-based regimens. The ROC analysis indicated good predictive accuracy with an area-under-the-curve of 0.69 (95% CI: 0.67-0.70). Before to each cycle of therapy, patients with risk scores ≥16 units would be considered at high risk for developing ≥grade 2 CINV.
The clinical application of this prediction tool will be an important source of individual patient risk information for the oncology clinician and may enhance patient care by optimizing the use of the antiemetics in a proactive manner.
尽管有有效的止吐药和循证指南,但高达40%接受化疗的癌症患者未能实现完全的恶心和呕吐控制。除了化疗类型外,还确定了几个与患者相关的化疗引起的恶心和呕吐(CINV)风险因素。为了将这些因素纳入预防性止吐药的最佳选择中,开发了一种基于重复测量周期的模型,用于预测化疗后第0至5天≥2级CINV(≥2次呕吐发作或因恶心导致口服摄入量减少)的风险。
汇总了参加五项非干预性CINV前瞻性研究之一的1198名患者的数据。在向后消除过程中使用广义估计方程,将P值设定为<0.05以识别相关预测因素。然后从最终模型系数中得出风险评分算法(范围0 - 32)。最后,进行了受试者操作特征曲线(ROCC)分析以测量评分算法的预测准确性。
在超过4197个化疗周期中,42.2%的患者经历了≥2级CINV。确定了八个风险因素:患者年龄<60岁、化疗的前两个周期、预期性恶心和呕吐、孕吐史、化疗前一晚的睡眠时间、前一周期的CINV、患者自行使用非处方治疗以及使用铂类或蒽环类方案。ROC分析表明预测准确性良好,曲线下面积为0.69(95%CI:0.67 - 0.70)。在每个治疗周期之前,风险评分≥16单位的患者将被视为发生≥2级CINV的高风险患者。
这种预测工具的临床应用将成为肿瘤临床医生获取个体患者风险信息的重要来源,并可能通过积极优化止吐药的使用来改善患者护理。