Delmas Clément, Conil Jean-Marie, Sztajnic Simon, Georges Bernard, Biendel Caroline, Dambrin Camille, Galinier Michel, Minville Vincent, Fourcade Olivier, Silva Stein, Marcheix Bertrand
Intensive Care Unit, Department of Anesthesia and Critical Care, University Hospital of Toulouse, Toulouse, France; Department of Cardiology, University Hospital of Rangueil, Toulouse, France.
Intensive Care Unit, Department of Anesthesia and Critical Care, University Hospital of Toulouse, Toulouse, France.
Indian J Crit Care Med. 2017 Mar;21(3):138-145. doi: 10.4103/ijccm.IJCCM_32_17.
Extracorporeal life support (ECLS) holds the promise of significant improvement of the survival of patient in refractory cardiogenic shock (CS) or cardiac arrest (CA). Nevertheless, it remains to be shown to which extent these highly invasive supportive techniques could improve long-term patient's outcome.
The outcomes of 82 adult ECLS patients at our institution between January 2012 and December 2013 were retrospectively analyzed.
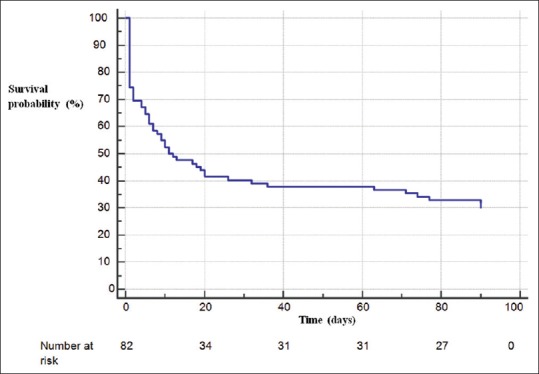
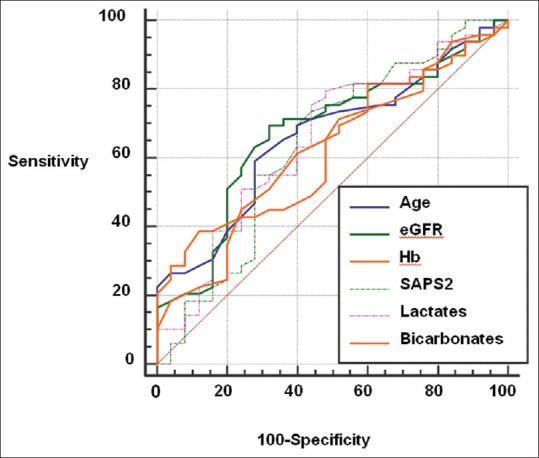
Patients were essentially men (64.7%) and are 54 years old. Preexisting ischemic (53.7%) and dilated cardiomyopathy (14.6%) were frequent. ECLS indications were shared equally between CA and CS. ECLS-specific adverse effects as hemorrhage (30%) and infection (50%) were frequent. ECLS was effective for 43 patients (54%) with recovery for 35 (43%), 5 (6%) heart transplant, and 3 (4%) left ventricular assist device support. Mortality rate at 30 days was 59.8%, but long-term and 3-month survival rates were similar of 31.7%. Initial plasma lactate levels >5.3 mmol/L and glomerular filtration rate <43 ml/min/1.73 m were significantly associated with 3-month mortality (risk ratio [RR] 2.58 [1.21-5.48]; = 0.014; RR 2.10 [1.1-4]; = 0.024, respectively). Long-term follow-up had shown patients paucisymptomatic (64% New York Heart Association 1-2) and autonomic (activities of daily living [ADL] score 6 ± 1.5).
In case of refractory CA or CS, lactates and renal function at ECLS initiation could serve as outcome predictor for risk stratification and ECLS indication.
体外生命支持(ECLS)有望显著提高难治性心源性休克(CS)或心脏骤停(CA)患者的生存率。然而,这些高侵入性支持技术在多大程度上能改善患者的长期预后仍有待证实。
回顾性分析了2012年1月至2013年12月在我院接受ECLS治疗的82例成年患者的预后情况。
患者以男性为主(64.7%),平均年龄54岁。既往存在缺血性心肌病(53.7%)和扩张型心肌病(14.6%)较为常见。CA和CS作为ECLS适应证的比例相当。ECLS特有的不良反应如出血(30%)和感染(50%)较为常见。43例患者(54%)ECLS治疗有效,其中35例(43%)恢复,5例(6%)接受心脏移植,3例(4%)接受左心室辅助装置支持。30天死亡率为59.8%,但长期生存率和3个月生存率相似,均为31.7%。初始血浆乳酸水平>5.3 mmol/L和肾小球滤过率<43 ml/min/1.73 m²与3个月死亡率显著相关(风险比[RR]分别为2.58[1.21 - 5.48];P = 0.014;RR 2.10[1.1 - 4];P = 0.024)。长期随访显示患者症状轻微(64%纽约心脏协会心功能分级1 - 2级)且自主能力良好(日常生活活动[ADL]评分6±1.5)。
对于难治性CA或CS,开始ECLS治疗时的乳酸水平和肾功能可作为风险分层及ECLS适应证的预后预测指标。