De Waal Reneé, Cohen Karen, Fox Matthew P, Stinson Kathryn, Maartens Gary, Boulle Andrew, Igumbor Ehimario U, Davies Mary-Ann
Centre for Infectious Disease Epidemiology and Research, School of Public Health and Family Medicine, University of Cape Town, Cape Town, South Africa.
Division of Clinical Pharmacology, Department of Medicine, University of Cape Town, Cape Town, South Africa.
J Int AIDS Soc. 2017 Apr 10;20(1):21317. doi: 10.7448/IAS.20.01/21317.
Tenofovir has been associated with decline in kidney function, but in patients with low baseline kidney function, improvements over time have been reported. Additionally, the magnitude and trajectory of estimated glomerular filtration rate (eGFR) changes may differ according to how eGFR is calculated. We described changes in eGFR over time, and the incidence of, and risk factors for, kidney toxicity, in a South African cohort.
We included antiretroviral-naïve patients ≥16 years old who started tenofovir-containing antiretroviral therapy (ART) between 2002 and 2013. We calculated eGFR using the Modification of Diet in Renal Disease (MDRD), Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI), and Cockcroft-Gault equations. We described changes in eGFR from ART initiation using linear mixed effects regression. We described the incidence of eGFR <30 mL/min on treatment, and identified associations with low eGFR using Cox regression.
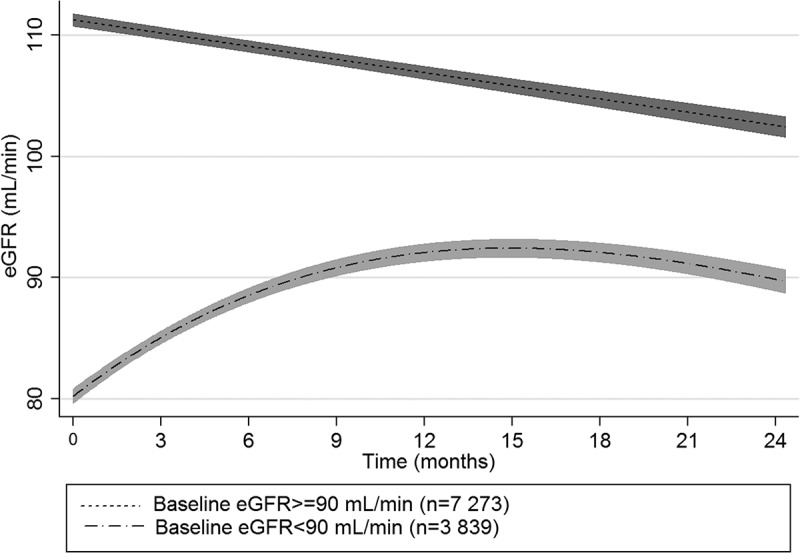
We included 15156 patients with median age of 35.4 years (IQR 29.9-42.0), median CD4 cell count of 168 cells/µL (IQR 83-243), and median eGFR (MDRD) of 98.6 mL/min (IQR 84.4-115.6). Median duration of follow up on tenofovir was 12.9 months (IQR 5.1-23.3). Amongst those with a baseline and subsequent eGFR available, mean eGFR change from baseline at 12 months was -4.4 mL/min (95% CI -4.9 to -4.0), -2.3 (-2.5 to -2.1), and 0.6 (0.04 to 1.2) in those with baseline eGFR ≥90 mL/min; and 11.9 mL/min (11.0 to 12.7), 14.6 (13.5 to 15.7), and 11.0 (10.3 to 11.7), in those with baseline eGFR <90 mL/min, according to the MDRD, CKD-EPI (n = 11 112), and Cockcroft-Gault (n = 9 283) equations, respectively. Overall, 292 (1.9%) patients developed eGFR <30 mL/min. Significant associations with low eGFR included older age, baseline eGFR <60 mL/min, CD4 count <200 cells/µL, body weight <60 kg, and concomitant protease inhibitor use.
Patients on tenofovir with baseline eGFR ≥90 mL/min experienced small but significant declines in eGFR over time when eGFR was estimated using the MDRD or CKD-EPI equations. However, eGFR increased in patients with eGFR <90 mL/min, regardless of which estimating equation was used. Decreases to below 30 mL/min were uncommon. In settings with limited access to laboratory testing, monitoring guidelines should consider focusing on higher risk patients.
替诺福韦与肾功能下降有关,但据报道,在基线肾功能较低的患者中,肾功能会随时间推移而改善。此外,根据估算肾小球滤过率(eGFR)的计算方法不同,其变化幅度和轨迹可能有所差异。我们描述了南非一个队列中eGFR随时间的变化情况,以及肾毒性的发生率和危险因素。
我们纳入了2002年至2013年间开始含替诺福韦抗逆转录病毒治疗(ART)的16岁及以上初治抗逆转录病毒患者。我们使用肾脏病饮食改良(MDRD)公式、慢性肾脏病流行病学合作(CKD-EPI)公式和Cockcroft-Gault公式计算eGFR。我们使用线性混合效应回归描述了从ART开始时eGFR的变化情况。我们描述了治疗期间eGFR<30 mL/min的发生率,并使用Cox回归确定与低eGFR的关联。
我们纳入了15156例患者,中位年龄为35.4岁(四分位间距29.9 - 42.0),中位CD4细胞计数为168个/µL(四分位间距83 - 243),中位eGFR(MDRD)为98.6 mL/min(四分位间距84.4 - 115.6)。替诺福韦的中位随访时间为12.9个月(四分位间距5.1 - 23.3)。在有基线和后续eGFR数据的患者中,根据MDRD公式、CKD-EPI公式(n = 11112)和Cockcroft-Gault公式(n = 9283),基线eGFR≥90 mL/min的患者在12个月时eGFR较基线的平均变化分别为-4.4 mL/min(95%置信区间-4.9至-4.0)、-2.3(-2.5至-2.1)和0.6(0.04至1.2);基线eGFR<90 mL/min的患者分别为11.9 mL/min(11.0至12.7)、14.6(13.5至15.7)和11.0(10.3至11.7)。总体而言,292例(1.9%)患者的eGFR<30 mL/min。与低eGFR显著相关的因素包括年龄较大、基线eGFR<60 mL/min、CD4计数<200个/µL、体重<60 kg以及同时使用蛋白酶抑制剂。
当使用MDRD或CKD-EPI公式估算eGFR时,基线eGFR≥90 mL/min的替诺福韦治疗患者的eGFR随时间出现了虽小但显著的下降。然而,无论使用哪种估算公式,eGFR<90 mL/min的患者其eGFR均有所升高。降至30 mL/min以下的情况并不常见。在实验室检测条件有限的环境中,监测指南应考虑重点关注高风险患者。