Department of Medicine, Indiana University School of Medicine, Indianapolis, Indiana.
Center for Biostatistics in AIDS Research, Harvard School of Public Health, Boston, Massachusetts.
Open Forum Infect Dis. 2014 Apr 16;1(1):ofu003. doi: 10.1093/ofid/ofu003. eCollection 2014 Mar.
The effects of antiretrovirals on cystatin C-based renal function estimates are unknown.
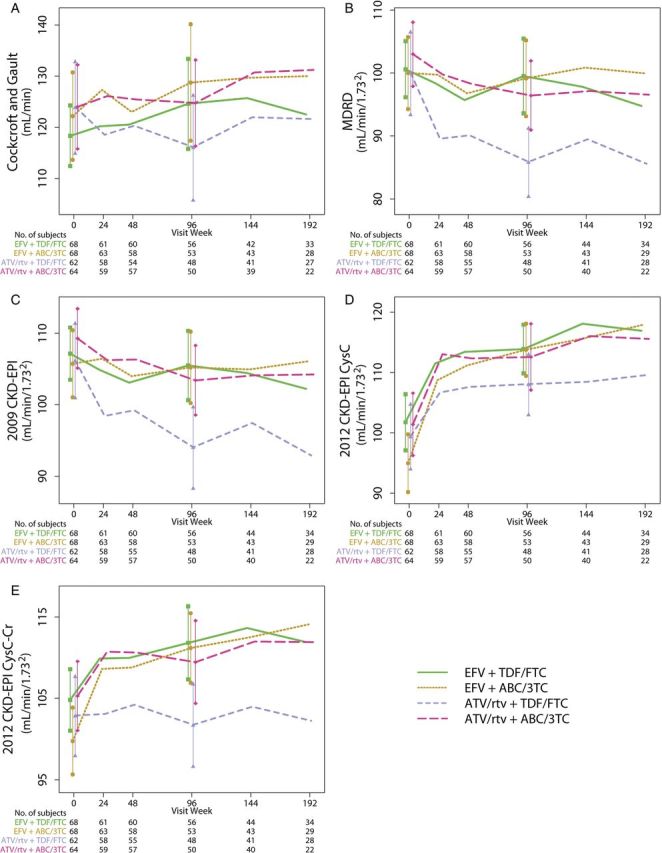
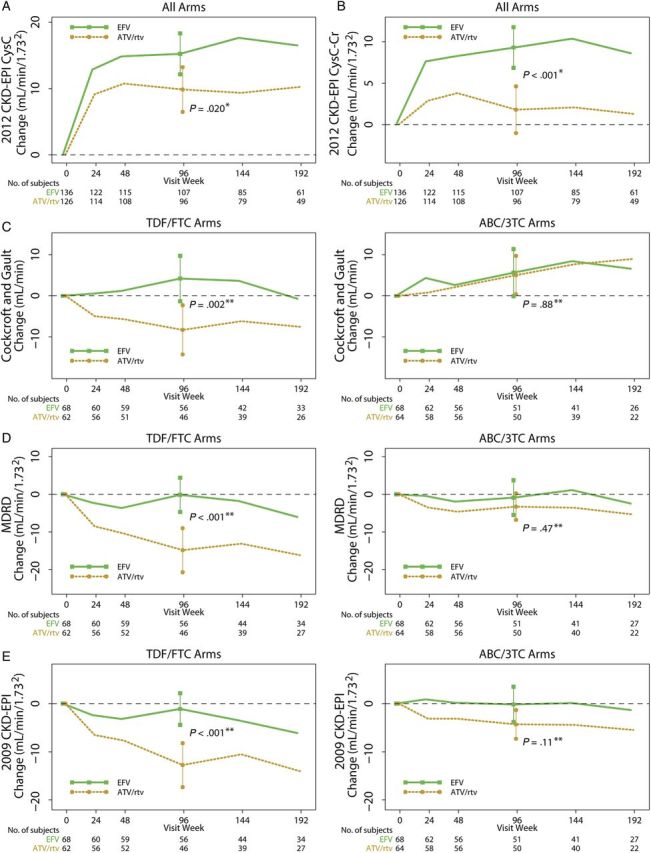
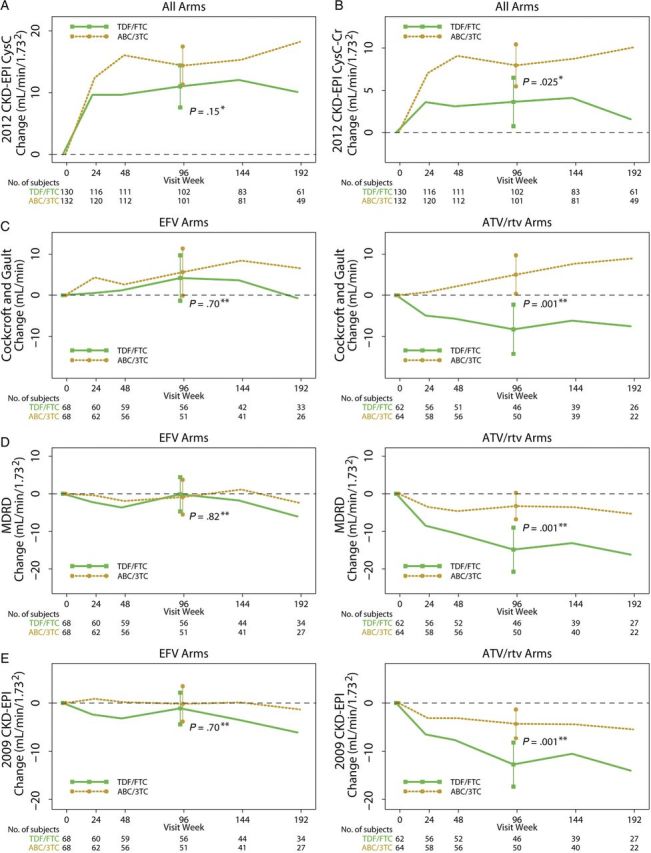
We analyzed changes in renal function using creatinine and cystatin C-based estimating equations in 269 patients in A5224s, a substudy of study A5202, in which treatment-naive patients were randomized to abacavir/lamivudine or tenofovir/emtricitabine with open-label atazanavir/ritonavir or efavirenz.
Changes in renal function significantly improved (or declined less) with abacavir/lamivudine treatment compared with tenofovir/emtricitabine using the Cockcroft-Gault formula (P = .016) and 2009 Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI; P = .030) and 2012 CKD-EPI cystatin C-creatinine (P = .025). Renal function changes significantly improved (or declined less) with efavirenz compared with atazanavir/ritonavir (P < .001 for all equations). Mean (95% confidence interval) renal function changes specifically for tenofovir/emtricitabine combined with atazanavir/ritonavir were -8.3 (-14.0, -2.6) mL/min with Cockcroft-Gault; -14.9 (-19.7, -10.1) mL/min per 1.73(2) with Modification of Diet in Renal Disease; -12.8 (-16.5, -9.0) mL/min per 1.73(2) with 2009 CKD-EPI; +8.9 (4.2, 13.7) mL/min per 1.73(2) with 2012 CKD-EPI cystatin C; and -1.2 (-5.1, 2.6) mL/min per 1.73(2) with 2012 CKD-EPI cystatin C-creatinine. Renal function changes for the other treatment arms were more favorable but similarly varied by estimating equation.
Antiretroviral-associated changes in renal function vary in magnitude and direction based on the estimating equation used.
目前尚不清楚抗逆转录病毒药物对基于半胱氨酸蛋白酶抑制剂 C 的肾功能估计值的影响。
我们分析了 269 例 A5224s 研究中的患者的肾功能变化,该研究为 A5202 研究的子研究,研究中,初治患者被随机分为阿巴卡韦/拉米夫定或替诺福韦/恩曲他滨,联合或不联合开放标签的阿扎那韦/利托那韦或依非韦伦治疗。
基于 Cockcroft-Gault 公式(P =.016)、2009 年慢性肾脏病流行病学合作组(CKD-EPI;P =.030)和 2012 年 CKD-EPI 半胱氨酸蛋白酶抑制剂 C-肌酐(P =.025),与替诺福韦/恩曲他滨相比,阿巴卡韦/拉米夫定治疗组肾功能变化明显改善(或下降较少)。与阿扎那韦/利托那韦相比,依非韦伦治疗组肾功能变化明显改善(所有方程 P <.001)。替诺福韦/阿扎那韦/利托那韦联合治疗组肾功能变化的平均值(95%置信区间)具体为:基于 Cockcroft-Gault 公式为-8.3(-14.0,-2.6)mL/min;基于改良肾脏病饮食研究公式为-14.9(-19.7,-10.1)mL/min/1.73(2);基于 2009 年 CKD-EPI 公式为-12.8(-16.5,-9.0)mL/min/1.73(2);基于 2012 年 CKD-EPI 半胱氨酸蛋白酶抑制剂 C 公式为+8.9(4.2,13.7)mL/min/1.73(2);基于 2012 年 CKD-EPI 半胱氨酸蛋白酶抑制剂 C-肌酐公式为-1.2(-5.1,2.6)mL/min/1.73(2)。其他治疗组的肾功能变化更有利,但因估算方程不同而变化。
基于所使用的估算方程,抗逆转录病毒相关的肾功能变化在幅度和方向上存在差异。