Hollingworth William, Busby John, Butler Christopher C, O'Brien Kathryn, Sterne Jonathan A C, Hood Kerenza, Little Paul, Lawton Michael, Birnie Kate, Thomas-Jones Emma, Harman Kim, Hay Alastair D
School of Social and Community Medicine, University of Bristol, Bristol, UK.
School of Social and Community Medicine, University of Bristol, Bristol, UK.
Value Health. 2017 Apr;20(4):556-566. doi: 10.1016/j.jval.2017.01.003. Epub 2017 Feb 22.
To estimate the cost-effectiveness of a two-step clinical rule using symptoms, signs and dipstick testing to guide the diagnosis and antibiotic treatment of urinary tract infection (UTI) in acutely unwell young children presenting to primary care.
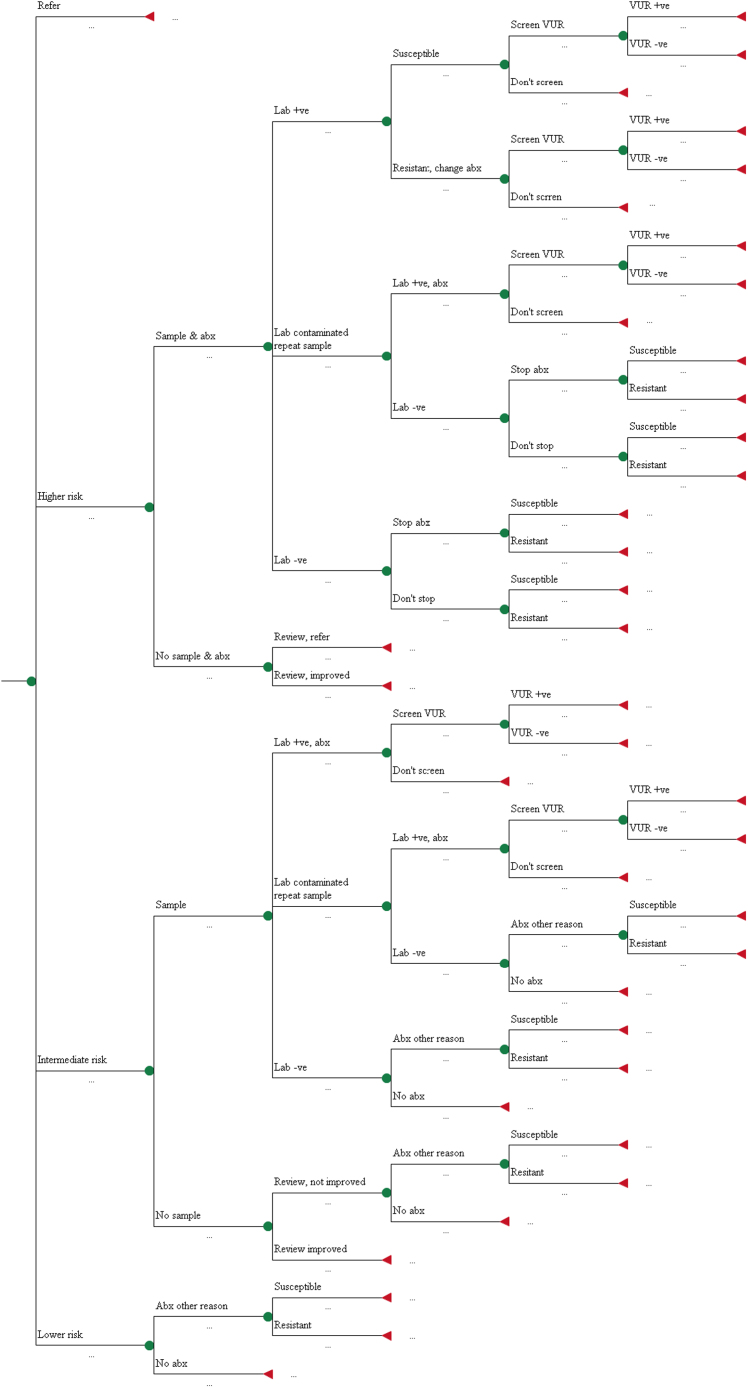
Decision analytic model synthesising data from a multicentre, prospective cohort study (DUTY) and the wider literature to estimate the short-term and lifetime costs and healthcare outcomes (symptomatic days, recurrent UTI, quality adjusted life years) of eight diagnostic strategies. We compared GP clinical judgement with three strategies based on a 'coefficient score' combining seven symptoms and signs independently associated with UTI and four strategies based on weighted scores according to the presence/absence of five symptoms and signs. We compared dipstick testing versus laboratory culture in children at intermediate risk of UTI.
Sampling, culture and antibiotic costs were lowest in high-specificity DUTY strategies (£1.22 and £1.08) compared to clinical judgement (£1.99). These strategies also approximately halved urine sampling (4.8% versus 9.1% in clinical judgement) without reducing sensitivity (58.2% versus 56.4%). Outcomes were very similar across all diagnostic strategies. High-specificity DUTY strategies were more cost-effective than clinical judgement in the short- (iNMB = £0.78 and £0.84) and long-term (iNMB =£2.31 and £2.50). Dipstick tests had poorer cost-effectiveness than laboratory culture in children at intermediate risk of UTI (iNMB = £-1.41).
Compared to GPs' clinical judgement, high specificity clinical rules from the DUTY study could substantially reduce urine sampling, achieving lower costs and equivalent patient outcomes. Dipstick testing children for UTI is not cost-effective.
评估一种两步临床规则的成本效益,该规则利用症状、体征和试纸检测来指导初级保健中急性不适幼儿的尿路感染(UTI)诊断及抗生素治疗。
决策分析模型综合了多中心前瞻性队列研究(DUTY)及更广泛文献的数据,以估计八种诊断策略的短期和终生成本及医疗保健结果(症状天数、复发性UTI、质量调整生命年)。我们将全科医生(GP)的临床判断与三种基于“系数评分”的策略进行比较,该评分结合了七个与UTI独立相关的症状和体征,还将其与四种基于五个症状和体征的存在与否的加权评分的策略进行比较。我们比较了UTI中度风险儿童的试纸检测与实验室培养。
与临床判断(1.99英镑)相比,高特异性DUTY策略的采样、培养和抗生素成本最低(分别为1.22英镑和1.08英镑)。这些策略还使尿液采样量减少了约一半(临床判断中为9.1%,而这里为4.8%),且未降低敏感性(分别为56.4%和58.2%)。所有诊断策略的结果非常相似。高特异性DUTY策略在短期(增量净货币效益[iNMB]=0.78英镑和0.84英镑)和长期(iNMB=2.31英镑和2.50英镑)比临床判断更具成本效益。在UTI中度风险儿童中,试纸检测的成本效益低于实验室培养(iNMB=-1.41英镑)。
与全科医生的临床判断相比,DUTY研究中的高特异性临床规则可大幅减少尿液采样,实现更低成本和相当的患者结果。对儿童进行UTI试纸检测不具有成本效益。