Department of Biostatistics and Epidemiology, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA, USA; Centre for Non-Communicable Diseases, Karachi, Pakistan.
Medical Research Council (MRC)/British Heart Foundation (BHF) Cardiovascular Epidemiology Unit, University of Cambridge, Cambridge, UK; MRC Integrative Epidemiology Unit, University of Bristol, Bristol, UK.
Lancet Diabetes Endocrinol. 2017 Jul;5(7):524-533. doi: 10.1016/S2213-8587(17)30088-8. Epub 2017 Apr 10.
The lipoprotein(a) pathway is a causal factor in coronary heart disease. We used a genetic approach to distinguish the relevance of two distinct components of this pathway, apolipoprotein(a) isoform size and circulating lipoprotein(a) concentration, to coronary heart disease.
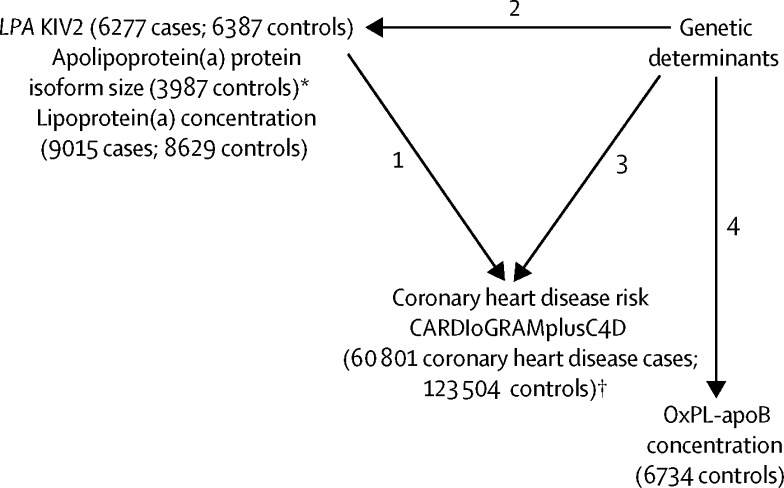
In this mendelian randomisation study, we measured lipoprotein(a) concentration and determined apolipoprotein(a) isoform size with a genetic method (kringle IV type 2 [KIV2] repeats in the LPA gene) and a serum-based electrophoretic assay in patients and controls (frequency matched for age and sex) from the Pakistan Risk of Myocardial Infarction Study (PROMIS). We calculated odds ratios (ORs) for myocardial infarction per 1-SD difference in either LPA KIV2 repeats or lipoprotein(a) concentration. In a genome-wide analysis of up to 17 503 participants in PROMIS, we identified genetic variants associated with either apolipoprotein(a) isoform size or lipoprotein(a) concentration. Using a mendelian randomisation study design and genetic data on 60 801 patients with coronary heart disease and 123 504 controls from the CARDIoGRAMplusC4D consortium, we calculated ORs for myocardial infarction with variants that produced similar differences in either apolipoprotein(a) isoform size in serum or lipoprotein(a) concentration. Finally, we compared phenotypic versus genotypic ORs to estimate whether apolipoprotein(a) isoform size, lipoprotein(a) concentration, or both were causally associated with coronary heart disease.
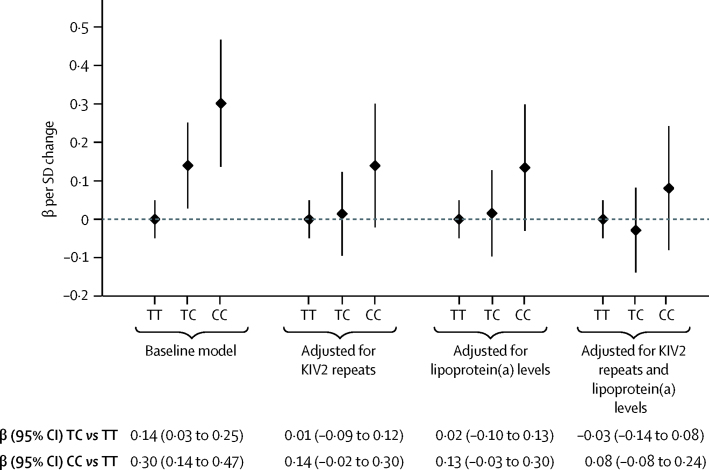
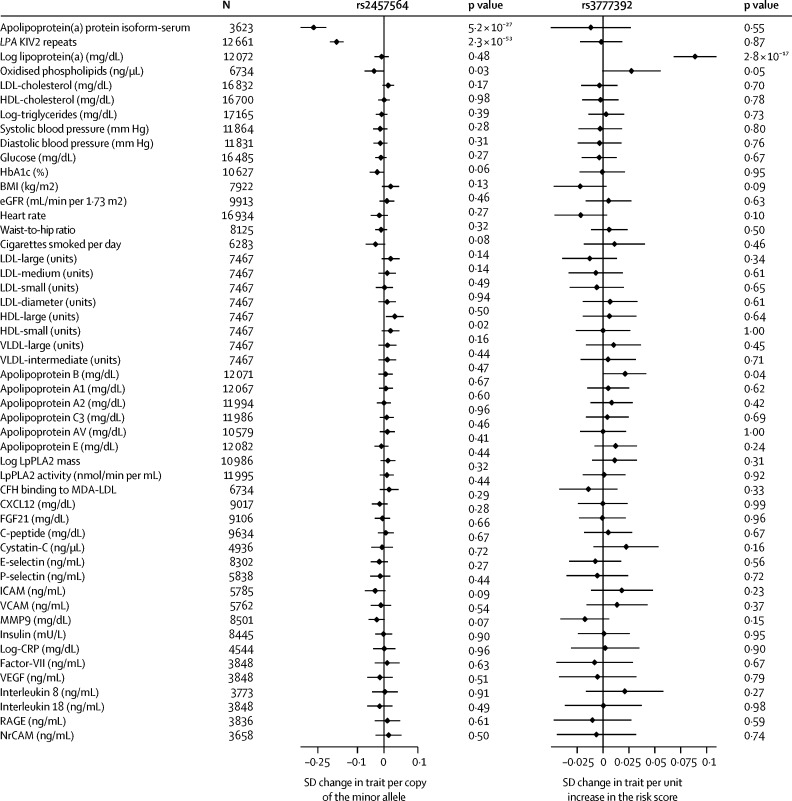
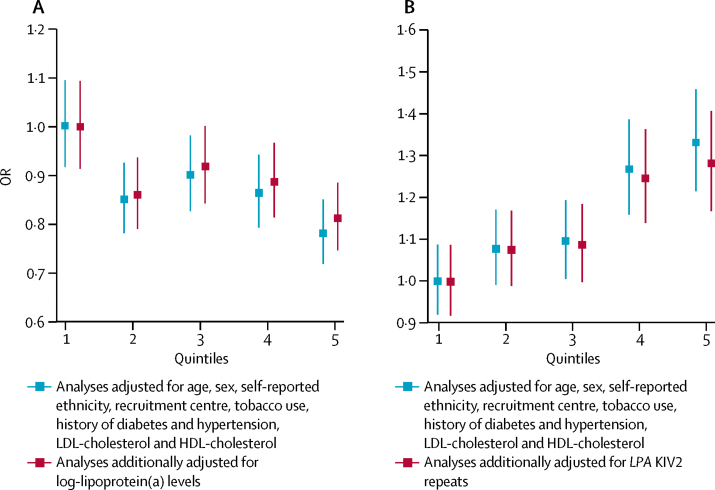
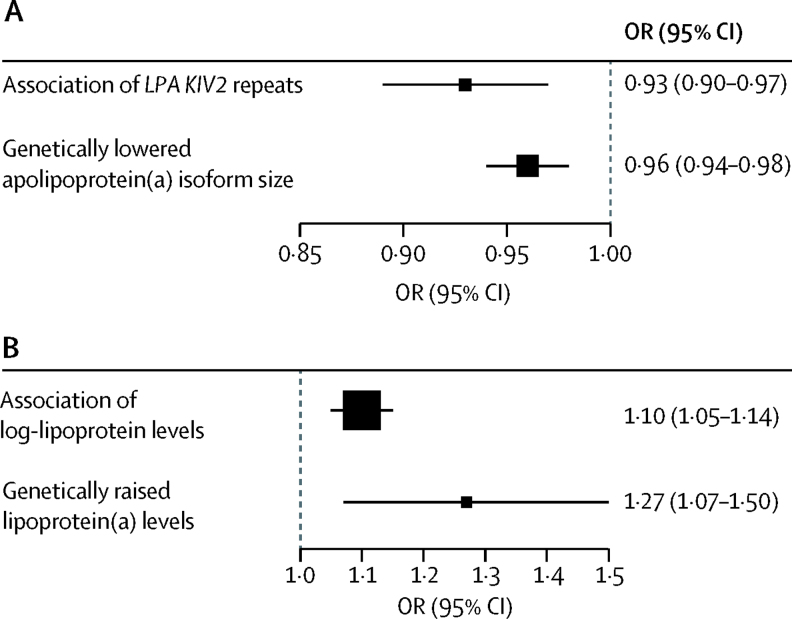
The PROMIS cohort included 9015 patients with acute myocardial infarction and 8629 matched controls. In participants for whom KIV2 repeat and lipoprotein(a) data were available, the OR for myocardial infarction was 0·93 (95% CI 0·90-0·97; p<0·0001) per 1-SD increment in LPA KIV2 repeats after adjustment for lipoprotein(a) concentration and conventional lipid concentrations. The OR for myocardial infarction was 1·10 (1·05-1·14; p<0·0001) per 1-SD increment in lipoprotein(a) concentration, after adjustment for LPA KIV2 repeats and conventional lipids. Genome-wide analysis identified rs2457564 as a variant associated with smaller apolipoprotein(a) isoform size, but not lipoprotein(a) concentration, and rs3777392 as a variant associated with lipoprotein(a) concentration, but not apolipoprotein(a) isoform size. In 60 801 patients with coronary heart disease and 123 504 controls, OR for myocardial infarction was 0·96 (0·94-0·98; p<0·0001) per 1-SD increment in apolipoprotein(a) protein isoform size in serum due to rs2457564, which was directionally concordant with the OR observed in PROMIS for a similar change. The OR for myocardial infarction was 1·27 (1·07-1·50; p=0·007) per 1-SD increment in lipoprotein(a) concentration due to rs3777392, which was directionally concordant with the OR observed for a similar change in PROMIS.
Human genetic data suggest that both smaller apolipoprotein(a) isoform size and increased lipoprotein(a) concentration are independent and causal risk factors for coronary heart disease. Lipoprotein(a)-lowering interventions could be preferentially effective in reducing the risk of coronary heart disease in individuals with smaller apolipoprotein(a) isoforms.
British Heart Foundation, US National Institutes of Health, Fogarty International Center, Wellcome Trust, UK Medical Research Council, UK National Institute for Health Research, and Pfizer.
载脂蛋白(a) 途径是冠心病的一个因果因素。我们使用遗传方法来区分该途径的两个不同成分,即载脂蛋白(a) 异构体大小和循环脂蛋白(a) 浓度,与冠心病的相关性。
在这项孟德尔随机研究中,我们测量了脂蛋白(a)浓度,并使用遗传方法(载脂蛋白(a)基因中的kringle IV 型 2 [KIV2] 重复)和血清电泳分析在来自巴基斯坦心肌梗死风险研究(PROMIS)的患者和对照者(按年龄和性别匹配)中确定载脂蛋白(a)异构体大小。我们计算了每标准差差异的心肌梗死比值比(OR),无论是在 LPA KIV2 重复还是脂蛋白(a)浓度方面。在 PROMIS 中对多达 17503 名参与者的全基因组分析中,我们确定了与载脂蛋白(a)异构体大小或脂蛋白(a)浓度相关的遗传变异。使用孟德尔随机研究设计和来自 CARDIOGRAMplusC4D 联盟的 60801 名冠心病患者和 123504 名对照者的遗传数据,我们计算了由于载脂蛋白(a)异构体大小在血清中的相似差异或脂蛋白(a)浓度而导致的心肌梗死的 OR。最后,我们比较了表型与基因型 OR,以估计载脂蛋白(a)异构体大小、脂蛋白(a)浓度或两者是否与冠心病有因果关系。
PROMIS 队列包括 9015 例急性心肌梗死患者和 8629 名匹配对照者。在有 KIV2 重复和脂蛋白(a)数据的参与者中,LPA KIV2 重复每增加 1-SD,心肌梗死的 OR 为 0.93(95%CI 0.90-0.97;p<0.0001),校正脂蛋白(a)浓度和常规脂质浓度后。脂蛋白(a)浓度每增加 1-SD,心肌梗死的 OR 为 1.10(1.05-1.14;p<0.0001),校正 LPA KIV2 重复和常规脂质后。全基因组分析确定 rs2457564 为与较小载脂蛋白(a)异构体大小相关但与脂蛋白(a)浓度无关的变异体,rs3777392 为与脂蛋白(a)浓度相关但与载脂蛋白(a)异构体大小无关的变异体。在 60801 名冠心病患者和 123504 名对照者中,由于 rs2457564,血清中载脂蛋白(a)蛋白异构体大小每增加 1-SD,心肌梗死的 OR 为 0.96(0.94-0.98;p<0.0001),这与 PROMIS 中观察到的类似变化的 OR 方向一致。由于 rs3777392,脂蛋白(a)浓度每增加 1-SD,心肌梗死的 OR 为 1.27(1.07-1.50;p=0.007),这与 PROMIS 中观察到的类似变化的 OR 方向一致。
人类遗传数据表明,较小的载脂蛋白(a)异构体大小和增加的脂蛋白(a)浓度都是冠心病的独立和因果危险因素。脂蛋白(a)降低干预措施可能更有效地降低载脂蛋白(a)异构体较小的个体患冠心病的风险。
英国心脏基金会、美国国立卫生研究院、福格蒂国际中心、惠康信托基金会、英国医学研究理事会、英国国家健康研究所和辉瑞公司。