Awoniyi Dolapo O, Baumann Ralf, Chegou Novel N, Kriel Belinda, Jacobs Ruschca, Kidd Martin, Loxton Andre G, Kaempfer Susanne, Singh Mahavir, Walzl Gerhard
DST/NRF Centre of Excellence for Biomedical TB Research and SAMRC Centre for TB Research, Division of Molecular Biology and Human Genetics, Department of Biomedical Sciences, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa.
Institute for Occupational and Social Medicine, Aachen University of Technology, Aachen, Germany.
Oncotarget. 2017 Jun 6;8(23):37525-37537. doi: 10.18632/oncotarget.16401.
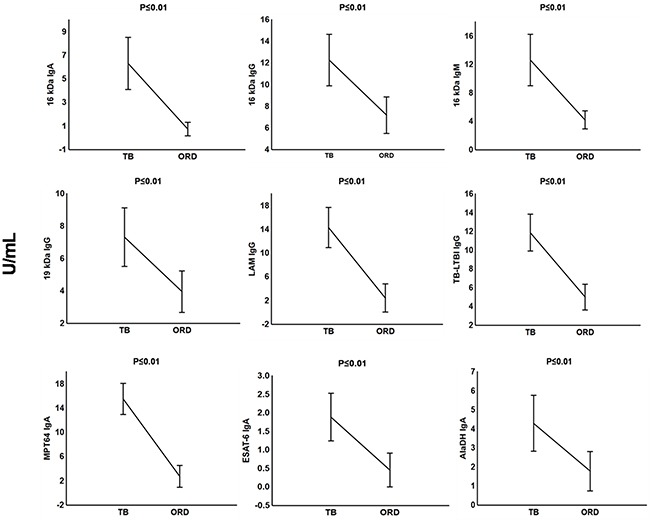
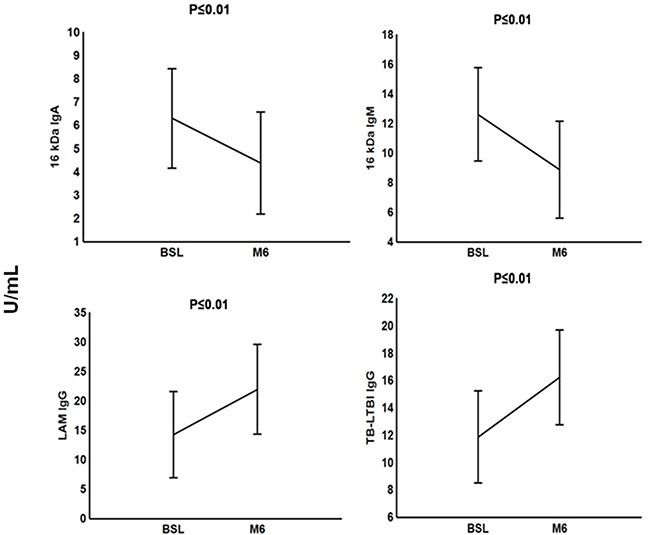
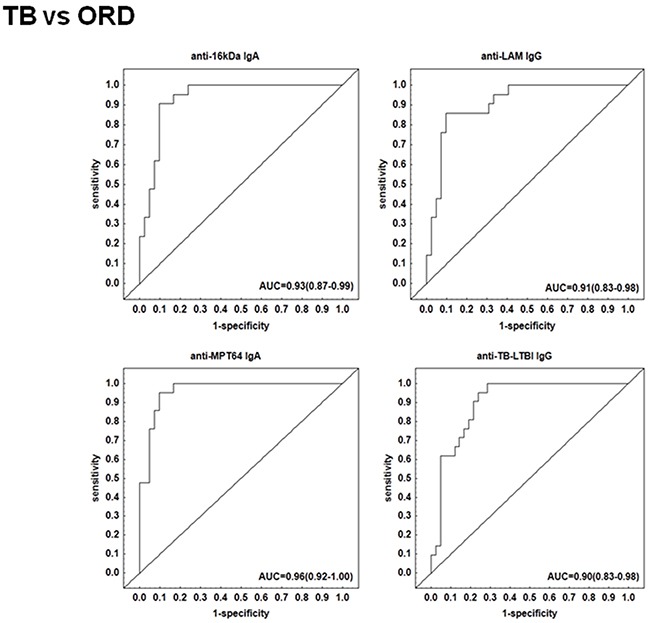
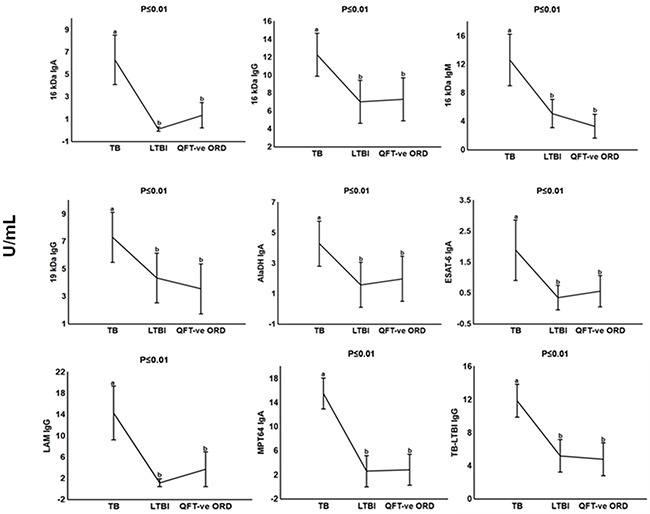
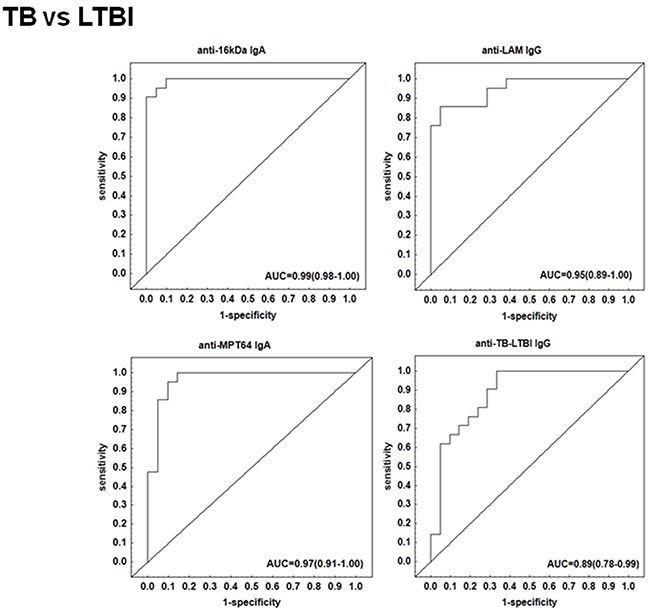
Immunoglobulin G (IgG) based tests for the diagnosis of active tuberculosis (TB) disease often show a lack of specificity in TB endemic regions, which is mainly due to a high background prevalence of LTBI. Here, we investigated the combined performance of the responses of different Ig classes to selected mycobacterial antigens in primary healthcare clinic attendees with signs and symptoms suggestive of TB. The sensitivity and specificity of IgA, IgG and/or IgM to LAM and 7 mycobacterial protein antigens (ESAT-6, Tpx, PstS1, AlaDH, MPT64, 16kDa and 19kDa) and 2 antigen combinations (TUB, TB-LTBI) in the plasma of 63 individuals who underwent diagnostic work-up for TB after presenting with symptoms and signs compatible with possible active TB were evaluated. Active TB was excluded in 42 individuals of whom 21 has LTBI whereas active TB was confirmed in 21 patients of whom 19 had a follow-up blood draw at the end of 6-month anti-TB treatment. The leading single serodiagnostic markers to differentiate between the presence or absence of active TB were anti-16 kDa IgA, anti-MPT64 IgA with sensitivity and specificity of 90%/90% and 95%/90%, respectively. The combined use of 3 or 4 antibodies further improved this performance to accuracies above 95%. After successful completion of anti-TB treatment at month 6, the levels of 16 kDa IgA and 16 kDa IgM dropped significantly whereas LAM IgG and TB-LTBI IgG increased. These results show the potential of extending investigation of anti-tuberculous IgG responses to include IgM and IgA responses against selected protein and non-protein antigens in differentiating active TB from other respiratory diseases in TB endemic settings.
基于免疫球蛋白G(IgG)的活动性结核病(TB)诊断检测在结核病流行地区往往缺乏特异性,这主要是由于潜伏性结核感染(LTBI)的背景患病率较高。在此,我们调查了在有结核病体征和症状的基层医疗诊所就诊者中,不同Ig类别对选定分枝杆菌抗原反应的综合性能。评估了63名出现与可能的活动性结核病相符的症状和体征后接受结核病诊断检查的个体血浆中IgA、IgG和/或IgM对脂阿拉伯甘露聚糖(LAM)和7种分枝杆菌蛋白抗原(早期分泌抗原靶6(ESAT-6)、硫氧还蛋白(Tpx)、磷酸蔗糖合成酶1(PstS1)、丙氨酸脱氢酶(AlaDH)、MPT64、16kDa和19kDa)以及2种抗原组合(TUB、TB-LTBI)的敏感性和特异性。42名个体被排除活动性结核病,其中21名有LTBI,而21名患者被确诊为活动性结核病,其中19名在6个月抗结核治疗结束时进行了随访采血。区分活动性结核病有无的主要单一血清学诊断标志物是抗16kDa IgA、抗MPT64 IgA,其敏感性和特异性分别为90%/90%和95%/90%。联合使用3种或4种抗体可进一步将此性能提高到95%以上的准确率。在第6个月抗结核治疗成功完成后,16kDa IgA和16kDa IgM水平显著下降,而LAM IgG和TB-LTBI IgG升高。这些结果表明,在结核病流行地区,扩大对抗结核IgG反应的研究以包括针对选定蛋白质和非蛋白质抗原的IgM和IgA反应,在区分活动性结核病与其他呼吸道疾病方面具有潜力。