Ragon Institute of Massachusetts General Hospital (MGH), Massachusetts Institute of Technology (MIT) and Harvard, Cambridge, MA, United States.
Division of Infectious Diseases, Brigham and Women's Hospital, Boston, MA, United States.
Front Immunol. 2022 Apr 20;13:856906. doi: 10.3389/fimmu.2022.856906. eCollection 2022.
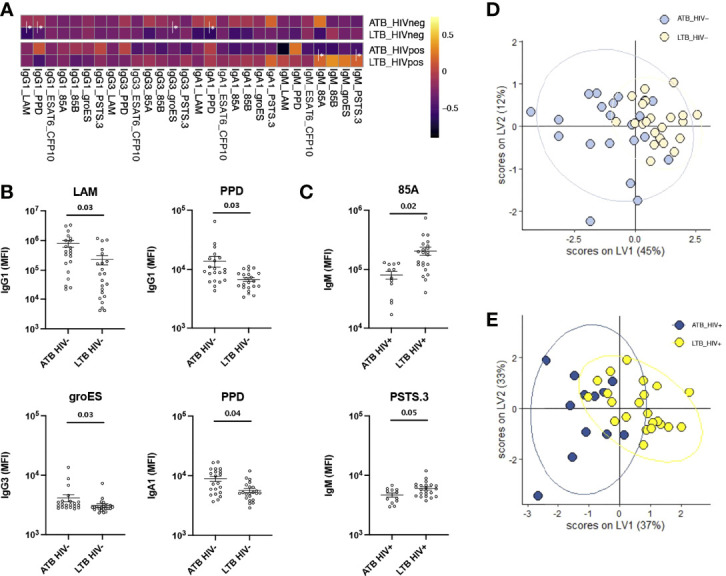
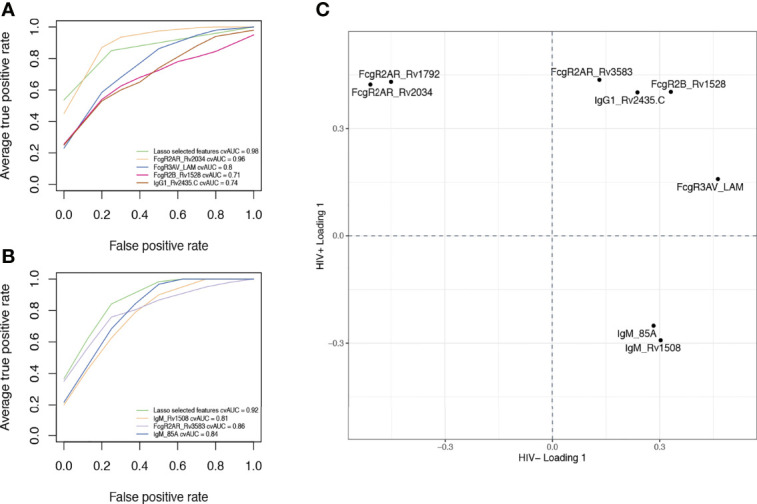
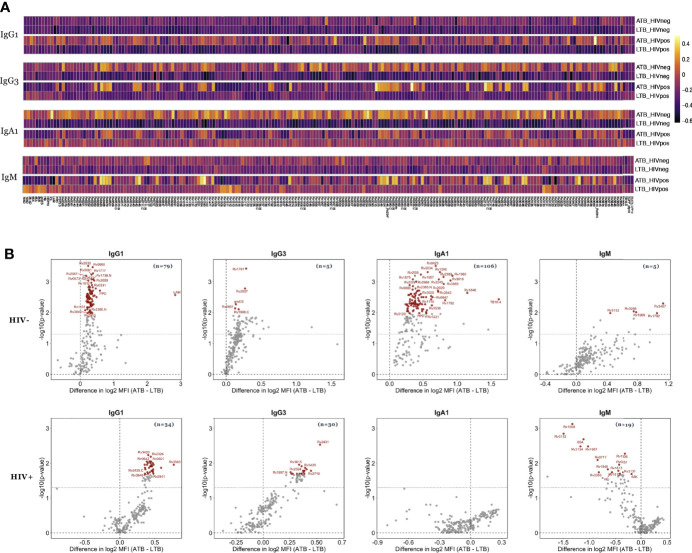
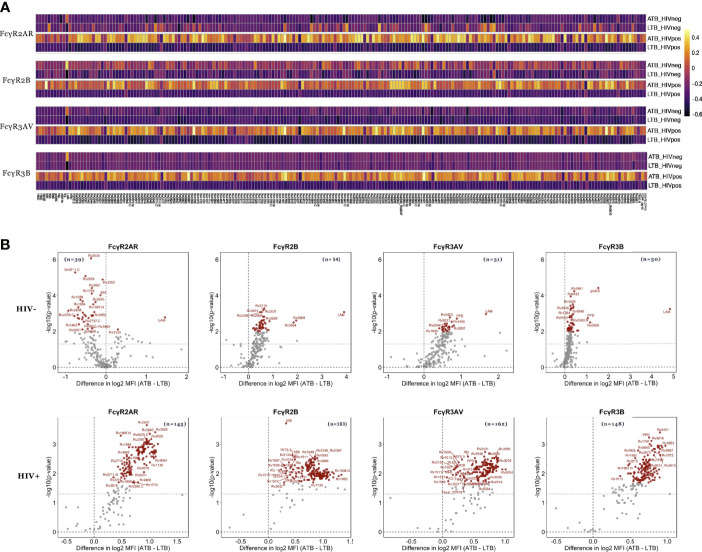
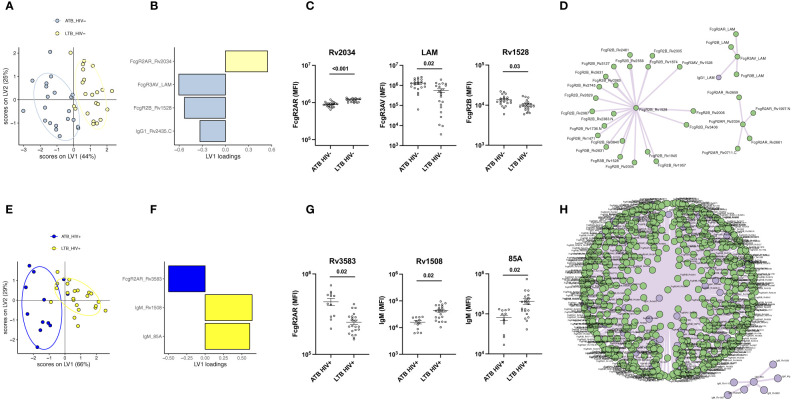
Tuberculosis (TB) is among the leading causes of death worldwide from a single infectious agent, second only to COVID-19 in 2020. TB is caused by infection with (Mtb), that results either in a latent or active form of disease, the latter associated with Mtb spread. In the absence of an effective vaccine, epidemiologic modeling suggests that aggressive treatment of individuals with active TB (ATB) may curb spread. Yet, clinical discrimination between latent (LTB) and ATB remains a challenge. While antibodies are widely used to diagnose many infections, the utility of antibody-based tests to diagnose ATB has only regained significant traction recently. Specifically, recent interest in the humoral immune response to TB has pointed to potential differences in both targeted antigens and antibody features that can discriminate latent and active TB. Here we aimed to integrate these observations and broadly profile the humoral immune response across individuals with LTB or ATB, with and without HIV co-infection, to define the most discriminatory humoral properties and diagnose TB disease more easily. Using 209 Mtb antigens, striking differences in antigen-recognition were observed across latently and actively infected individuals that was modulated by HIV serostatus. However, ATB and LTB could be discriminated, irrespective of HIV-status, based on a combination of both antibody levels and Fc receptor-binding characteristics targeting both well characterized (like lipoarabinomannan, 38 kDa or antigen 85) but also novel Mtb antigens (including Rv1792, Rv1528, Rv2435C or Rv1508). These data reveal new Mtb-specific immunologic markers that can improve the classification of ATB versus LTB.
结核病 (TB) 是全球由单一感染源导致的主要死亡原因之一,仅次于 2020 年的 COVID-19。结核病是由感染引起的 (Mtb),导致疾病的潜伏或活跃形式,后者与 Mtb 的传播有关。在没有有效疫苗的情况下,流行病学模型表明,积极治疗活动性结核病 (ATB) 患者可能会遏制传播。然而,临床区分潜伏性 (LTB) 和 ATB 仍然是一个挑战。虽然抗体广泛用于诊断许多感染,但基于抗体的测试用于诊断 ATB 的效用最近才重新受到关注。具体来说,最近对结核病体液免疫反应的兴趣指出,潜在和活跃的结核病在靶向抗原和抗体特征方面可能存在潜在差异,这些差异可以区分潜伏性和活动性结核病。在这里,我们旨在整合这些观察结果,并广泛分析 LTB 或 ATB 个体以及伴有或不伴有 HIV 合并感染的个体的体液免疫反应,以确定最具鉴别力的体液特性,并更轻松地诊断结核病。使用 209 种 Mtb 抗原,在潜伏和感染个体中观察到针对抗原的识别存在显著差异,这种差异受 HIV 血清状态调节。然而,无论 HIV 状况如何,都可以根据针对多种抗原的抗体水平和 Fc 受体结合特性的组合来区分 ATB 和 LTB,这些抗原既包括特征明确的抗原(如脂阿拉伯甘露聚糖、38 kDa 或抗原 85),也包括新型 Mtb 抗原(包括 Rv1792、Rv1528、Rv2435C 或 Rv1508)。这些数据揭示了新的 Mtb 特异性免疫标志物,可以改善 ATB 与 LTB 的分类。