Groisberg Roman, Hong David S, Holla Vijaykumar, Janku Filip, Piha-Paul Sarina, Ravi Vinod, Benjamin Robert, Kumar Patel Shreyas, Somaiah Neeta, Conley Anthony, Ali Siraj M, Schrock Alexa B, Ross Jeffrey S, Stephens Philip J, Miller Vincent A, Sen Shiraj, Herzog Cynthia, Meric-Bernstam Funda, Subbiah Vivek
Department of Investigational Cancer Therapeutics (A Phase I Program), Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, Houston, Texas 77030, USA.
Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, Houston, Texas 77030, USA.
Oncotarget. 2017 Jun 13;8(24):39254-39267. doi: 10.18632/oncotarget.16845.
There are currently no United States Food and Drug Administration approved molecularly matched therapies for sarcomas except gastrointestinal stromal tumors. Complicating this is the extreme diversity, heterogeneity, and rarity of these neoplasms. Few therapeutic options exist for relapsed and refractory sarcomas. In clinical practice many oncologists refer patients for genomic profiling hoping for guidance on treatment options after standard therapy. However, a systematic analysis of actionable mutations has yet to be completed. We analyzed genomic profiling results in patients referred to MD Anderson Cancer Center with advanced sarcomas to elucidate the frequency of potentially actionable genomic alterations in this population.
We reviewed charts of patients with advanced sarcoma who were referred to investigational cancer therapeutics department and had CLIA certified comprehensive genomic profiling (CGP) of 236 or 315 cancer genes in at least 50ng of DNA. Actionable alterations were defined as those identifying anti-cancer drugs on the market, in registered clinical trials, or in the Drug-Gene Interaction Database.
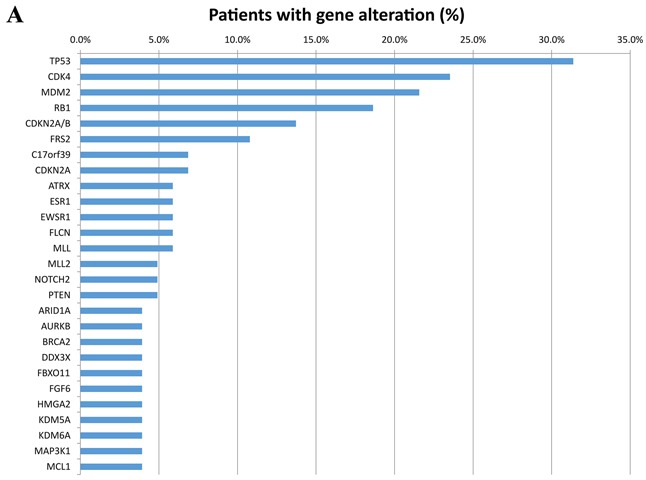
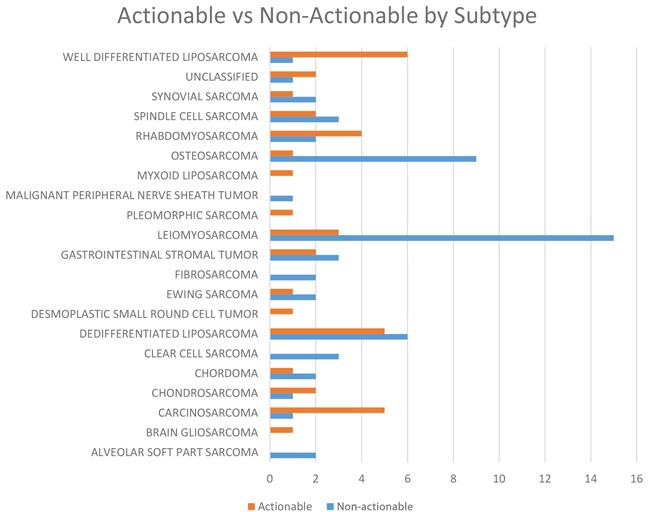
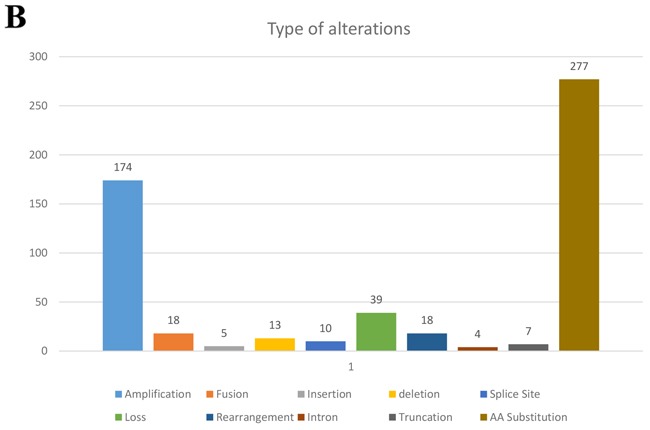
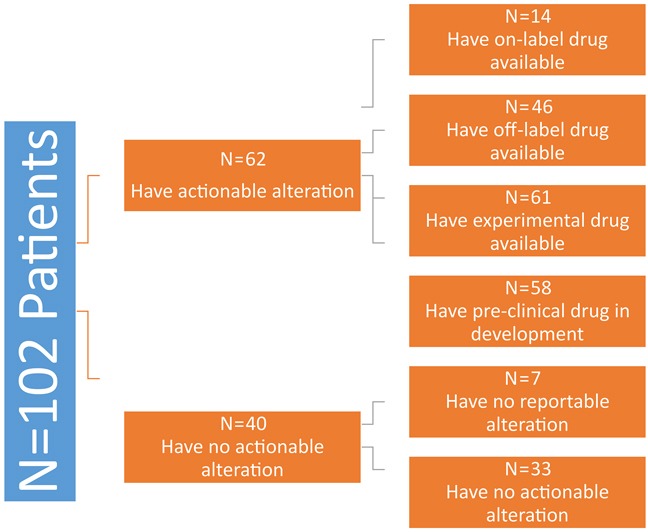
Among the 102 patients analyzed median age was 45.5 years (range 8-76), M: F ratio 48:54. The most common subtypes seen in our study were leiomyosarcoma (18.6%), dedifferentiated liposarcoma (11%), osteosarcoma (11%), well-differentiated liposarcoma (7%), carcinosarcoma (6%), and rhabdomyosarcoma (6%). Ninety-five out of 102 patients (93%) had at least one genomic alteration identified with a mean of six mutations per patient. Of the 95 biopsy samples with identifiable genomic alterations, the most commonly affected genes were TP53 (31.4%), CDK4 (23.5%), MDM2 (21.6%), RB1 (18.6%), and CDKN2A/B (13.7%). Notable co-segregating amplifications included MDM2-CDK4 and FRS2-FGF. Sixteen percent of patients received targeted therapy based on CGP of which 50% had at least stable disease.
Incorporating CGP into sarcoma management may allow for more precise diagnosis and sub-classification of this diverse and rare disease, as well as personalized matching of patients to targeted therapies such as those available in basket clinical trials.
除胃肠道间质瘤外,目前美国食品药品监督管理局尚未批准针对肉瘤的分子匹配疗法。这些肿瘤具有极度的多样性、异质性和罕见性,使情况更为复杂。复发和难治性肉瘤的治疗选择很少。在临床实践中,许多肿瘤学家会让患者进行基因组分析,希望能在标准治疗后获得治疗方案的指导。然而,尚未完成对可操作突变的系统分析。我们分析了转诊至MD安德森癌症中心的晚期肉瘤患者的基因组分析结果,以阐明该人群中潜在可操作的基因组改变的频率。
我们回顾了转诊至癌症治疗研究部门的晚期肉瘤患者的病历,这些患者对至少50纳克DNA中的236个或315个癌症基因进行了经临床实验室改进修正案(CLIA)认证的全面基因组分析(CGP)。可操作的改变被定义为那些在市场上、注册临床试验中或药物-基因相互作用数据库中可识别抗癌药物的改变。
在分析的102例患者中,中位年龄为45.5岁(范围8 - 76岁),男女比例为48:54。我们研究中最常见的亚型是平滑肌肉瘤(18.6%)、去分化脂肪肉瘤(11%)、骨肉瘤(11%)、高分化脂肪肉瘤(7%)、癌肉瘤(6%)和横纹肌肉瘤(6%)。102例患者中有95例(93%)至少有一处基因组改变,平均每位患者有6处突变。在95份具有可识别基因组改变的活检样本中,最常受影响的基因是TP53(31.4%)、CDK4(23.5%)、MDM2(21.6%)、RB1(18.6%)和CDKN2A/B(13.7%)。值得注意的共分离扩增包括MDM2 - CDK4和FRS2 - FGF。16%的患者基于CGP接受了靶向治疗,其中50%至少病情稳定。
将CGP纳入肉瘤管理可能有助于对这种多样且罕见的疾病进行更精确的诊断和亚分类,以及为患者进行个性化的靶向治疗匹配,例如篮式临床试验中可用的治疗方法。