Kim Dae Keun, Parihar Jaspreet Singh, Kwon Young Suk, Kim Sinae, Shinder Brian, Lee Nara, Farber Nicholas, Ahlering Thomas, Skarecky Douglas, Yuh Bertram, Ruel Nora, Kim Wun-Jae, Rha Koon Ho, Kim Isaac Yi
Department of Urology, CHA Seoul Station Medical Center, CHA University, CHA Medical School, Seoul 04637, Korea.
Department of Urology, School of Medicine, Graduate School, Hanyang University, Seoul 04763, Korea.
Asian J Androl. 2018 Jan-Feb;20(1):9-14. doi: 10.4103/1008-682X.196852.
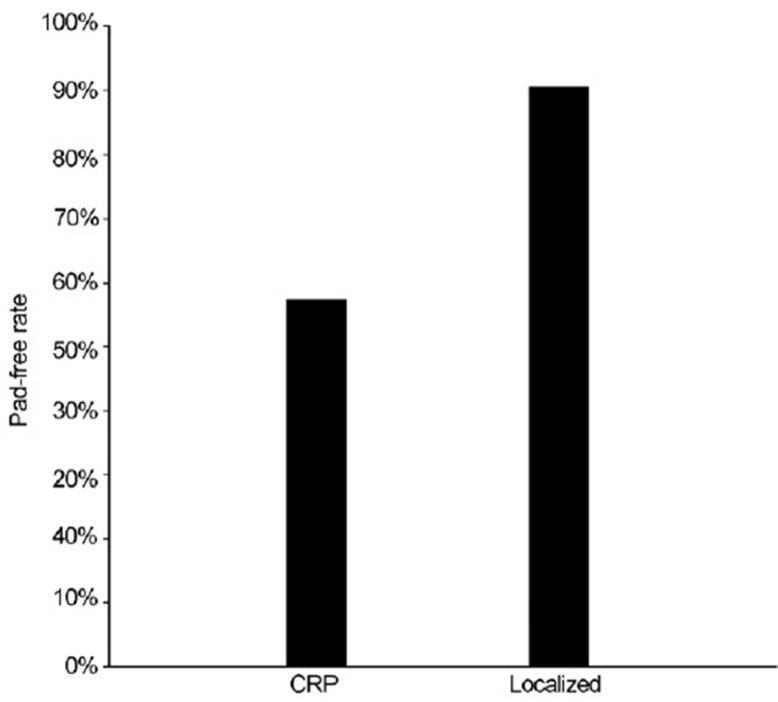
Emerging evidence has suggested that cytoreductive prostatectomy (CRP) allows superior oncologic control when compared to current standard of care androgen deprivation therapy alone. However, the safety and benefit of cytoreduction in metastatic prostate cancer (mPCa) has not been proven. Therefore, we evaluated the incidence of complications following CRP in men newly diagnosed with mPCa. A total of 68 patients who underwent CRP from 2006 to 2014 at four tertiary surgical centers were compared to 598 men who underwent radical prostatectomy for clinically localized prostate cancer (PCa). Urinary incontinence was defined as the use of any pad. CRP had longer operative times (200 min vs 140 min, P < 0.0001) and higher estimated blood loss (250 ml vs 125 ml, P < 0.0001) compared to the control group. However, both overall (8.82% vs 5.85%) and major complication rates (4.41% vs 2.17%) were comparable between the two groups. Importantly, urinary incontinence rate at 1-year after surgery was significantly higher in the CRP group (57.4% vs 90.8%, P < 0.0001). Univariate logistic analysis showed that the estimated blood loss was the only independent predictor of perioperative complications both in the unadjusted model (OR: 1.18; 95% CI: 1.02-1.37; P = 0.025) and surgery type-adjusted model (OR: 1.17; 95% CI: 1.01-1.36; P = 0.034). In conclusion, CRP is more challenging than radical prostatectomy and associated with a notably higher incidence of urinary incontinence. Nevertheless, CRP is a technically feasible and safe surgery for selecting PCa patients who present with node-positive or bony metastasis when performed by experienced surgeons. A prospective, multi-institutional clinical trial is currently underway to verify this concept.
新出现的证据表明,与目前单纯雄激素剥夺疗法的标准治疗相比,减瘤性前列腺切除术(CRP)能实现更好的肿瘤控制。然而,转移性前列腺癌(mPCa)中减瘤的安全性和益处尚未得到证实。因此,我们评估了新诊断为mPCa的男性患者接受CRP后的并发症发生率。将2006年至2014年在四个三级外科中心接受CRP的68例患者与598例因临床局限性前列腺癌(PCa)接受根治性前列腺切除术的男性患者进行比较。尿失禁定义为使用任何尿垫。与对照组相比,CRP的手术时间更长(200分钟对140分钟,P<0.0001),估计失血量更高(250毫升对125毫升,P<0.0001)。然而,两组的总体并发症发生率(8.82%对5.85%)和主要并发症发生率(4.41%对2.17%)相当。重要的是,CRP组术后1年的尿失禁率显著更高(57.4%对90.8%,P<0.0001)。单因素逻辑分析表明,估计失血量是未调整模型(OR:1.18;95%CI:1.02-1.37;P=0.025)和手术类型调整模型(OR:1.17;95%CI:1.01-1.36;P=0.034)中围手术期并发症的唯一独立预测因素。总之,CRP比根治性前列腺切除术更具挑战性,且尿失禁发生率明显更高。然而,对于有经验的外科医生来说,CRP对于选择出现淋巴结阳性或骨转移的PCa患者是一种技术上可行且安全的手术。目前正在进行一项前瞻性、多机构的临床试验来验证这一概念。