Xue Peng, Wu Ziyu, Wang Kunpen, Gao Guojun, Zhuang Min, Yan Miao
Department of Urology, First People Hospital of Lianyungang, Lianyungang, Jiangsu Province, People's Republic of China.
Department of Urology, NO 2 Hospital of Huaian, Huaian, Jiangsu Province, People's Republic of China.
Cancer Manag Res. 2020 Sep 23;12:8867-8873. doi: 10.2147/CMAR.S270882. eCollection 2020.
The current standard of care for metastatic prostate cancer (mPCa) is androgen deprivation therapy (ADT) with or without anti-androgen and chemotherapy. The aim of this study was to evaluate the efficacy and safety of a multimodal approach including local primary tumor therapy, metastasis-directed therapy (MDT), and hormonal therapy in patients with oligometastatic prostate cancer (PCa).
We reviewed data of patients with PCa and bone oligometastases at diagnosis treated in three institutions with ADT followed by cytoreductive surgery with or without metastases-directed radiotherapy. Oligometastases were defined as the presence of five or fewer metastatic lesions with the absence of visceral metastases. In this retrospective cohort study, 58 patients underwent cytoreductive radical prostatectomy and ADT. Of these, 26 patients (45%) received stereotactic body radiation therapy (SBRT) to all metastatic sites as a MDT. Oncological outcomes were analyzed using the Kaplan-Meier method.
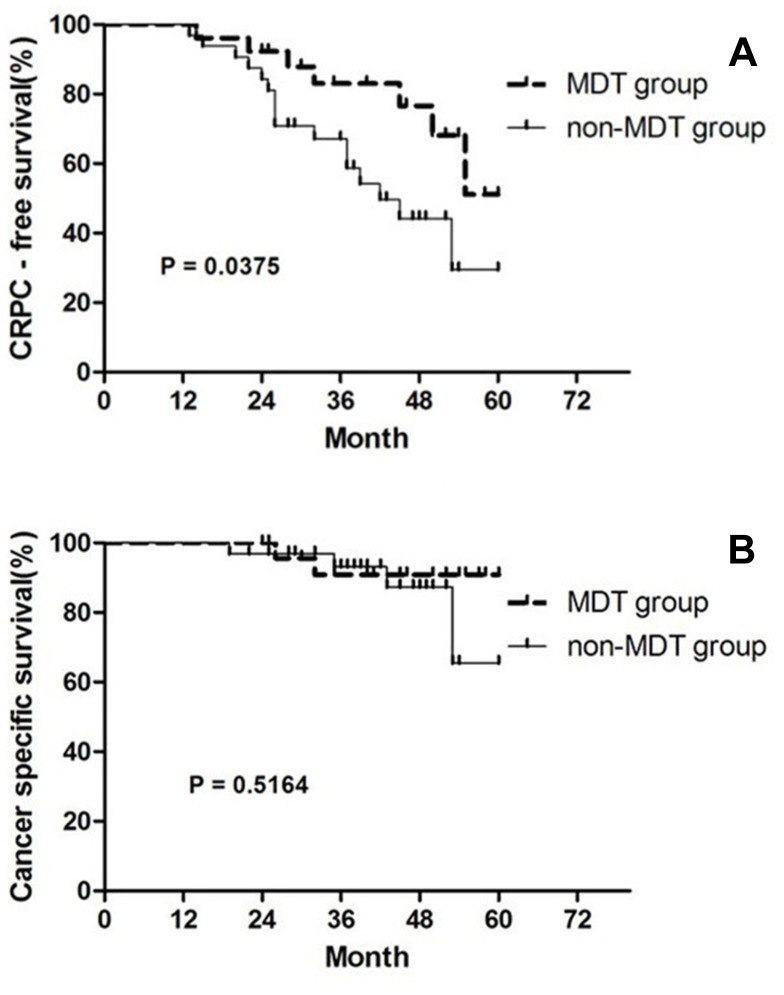
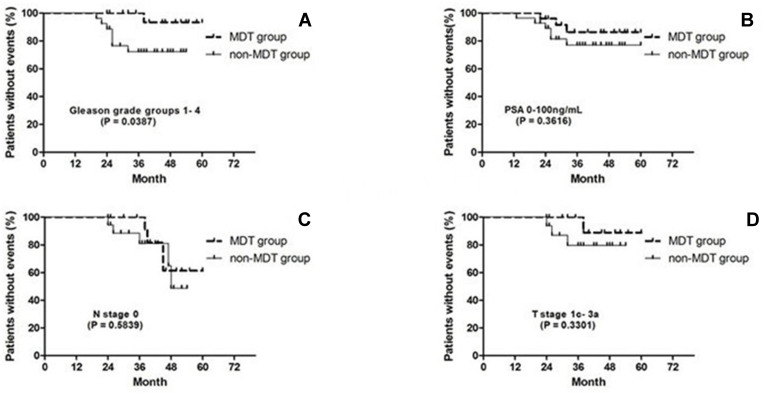
The median follow-up period was 46.2 months. Of the 58 patients, the 3-year castration-resistant prostate cancer (CRPC)-free survival and cancer-specific survival was 75.9% and 91.4%, respectively. Pre- or post-treatment predictive factors for progression to CRPC, including prostate-specific antigen (PSA) level at diagnosis ≥20 ng/mL, Gleason grade groups 5, clinical T stage cT3b-4, PSA nadir level of ≥0.05 ng/mL, and no MDT with SBRT, were significantly associated with progression to CRPC. Subgroup analysis showed that the MDT group had significantly better CRPC-free survival than the non-MDT group with Gleason grade groups 1-4 (HR=0.228; 95% CI= 0.056-0.926). A total of 3.4% of the patients had grade 2 acute genitourinary toxicities and 5.2% had grade 2 acute gastrointestinal toxicities. No late grade >2 adverse events were observed.
This multi-center, retrospective cohort study revealed the feasibility of combining cytoreductive prostatectomy and metastasis-directed radiotherapy for newly-diagnosed oligometastatic PCa. This treatment strategy has the potential to delay the progression to CRPC.
转移性前列腺癌(mPCa)目前的标准治疗方法是雄激素剥夺疗法(ADT),可联合或不联合抗雄激素药物及化疗。本研究的目的是评估多模式治疗方法在寡转移性前列腺癌(PCa)患者中的疗效和安全性,该方法包括局部原发性肿瘤治疗、转移灶定向治疗(MDT)和激素治疗。
我们回顾了在三家机构接受治疗的PCa和诊断时伴有骨寡转移患者的数据,这些患者先接受ADT治疗,随后接受减瘤手术,部分患者还接受了或未接受转移灶定向放疗。寡转移定义为存在五个或更少的转移病灶且无内脏转移。在这项回顾性队列研究中,58例患者接受了减瘤性前列腺癌根治术和ADT治疗。其中,26例患者(45%)接受了立体定向体部放疗(SBRT),作为MDT用于所有转移部位。采用Kaplan-Meier方法分析肿瘤学结局。
中位随访期为46.2个月。在这58例患者中,3年无去势抵抗性前列腺癌(CRPC)生存率和癌症特异性生存率分别为75.9%和91.4%。进展为CRPC的治疗前或治疗后预测因素,包括诊断时前列腺特异性抗原(PSA)水平≥20 ng/mL、Gleason分级5级、临床T分期cT3b-4、PSA最低点水平≥0.05 ng/mL以及未接受SBRT的MDT,均与进展为CRPC显著相关。亚组分析显示,对于Gleason分级1-4级的患者,MDT组的无CRPC生存率显著高于非MDT组(HR=0.228;95%CI=0.056-0.926)。共有3.4%的患者出现2级急性泌尿生殖系统毒性反应,5.2%的患者出现2级急性胃肠道毒性反应。未观察到晚期大于2级的不良事件。
这项多中心回顾性队列研究揭示了将减瘤性前列腺切除术和转移灶定向放疗相结合用于新诊断的寡转移性PCa的可行性。这种治疗策略有可能延缓进展为CRPC。