Ng Yue-Harn, Ganta Kavitha, Davis Herbert, Pankratz V Shane, Unruh Mark
Division of Nephrology, Department of Internal Medicine, University of New Mexico, Albuquerque, NM, USA.
New Mexico VA Health Care System, Albuquerque, NM, USA.
Front Med (Lausanne). 2017 Apr 11;4:40. doi: 10.3389/fmed.2017.00040. eCollection 2017.
Acute kidney injury requiring renal replacement therapy (RRT) in the intensive care unit portends a poor prognosis. The decisions regarding dialysis catheter placement is based mainly on physician discretion with little evidence to support the choice of dialysis catheter location.
The Veterans Affairs/National Institutes of Health Acute Renal Failure Trial Network Study was a multicenter, prospective, randomized trial of intensive vs. less intensive RRT in critically ill patients with AKI. We assessed the association of dialysis catheter location with dialysis catheter-related outcomes including catheter-related complications, mortality, dialysis dependence, and dialysis dose delivered.
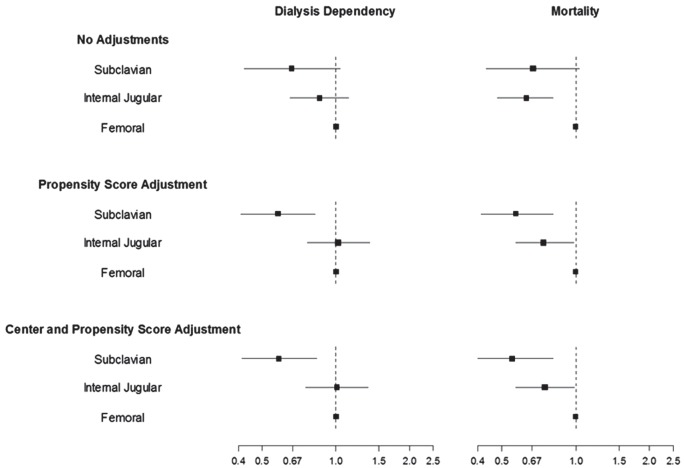
Of the 1,124 patients enrolled in the ATN study, catheter data were available in 1,016 (90.39%) patients. A total of 91 (8.96%) subclavian, 387 (38.09%) internal jugular, and 538 (52.95%) femoral dialysis catheters were inserted. The femoral group was younger (58.39 ± 16.27), had greater bleeding tendency [lower platelet count (96.00 ± 109.35) with higher INR (2.01 ± 2.19)], and had a higher baseline sequential organ failure assessment score on admission (14.59 ± 3.61) compared to the other two groups. Dialysis catheter-related complications were low in this study with no significant difference in the rates of complications among all catheter locations. Mortality and dialysis dependence was lowest in the subclavian group, while the dose of dialysis delivered (Kt/V) remained lowest in the femoral group, after propensity score and center adjustments.
Patient characteristics influence the choice of dialysis catheter location with a tendency to place femoral catheters in younger, sicker, and more coagulopathic patients. There were no statistically significant differences in complication rates among the three catheter locations, although femoral catheters may be associated with a lower delivered dose of dialysis during intermittent hemodialysis.
www.ClinicalTrials.gov, identifier NCT00076219.
在重症监护病房中,需要进行肾脏替代治疗(RRT)的急性肾损伤预示着预后不良。关于透析导管置入的决策主要基于医生的判断,几乎没有证据支持透析导管位置的选择。
退伍军人事务部/国立卫生研究院急性肾衰竭试验网络研究是一项针对急性肾损伤危重症患者进行强化与非强化RRT的多中心、前瞻性、随机试验。我们评估了透析导管位置与透析导管相关结局的关联,包括导管相关并发症、死亡率、透析依赖以及透析剂量。
在急性肾小管坏死(ATN)研究纳入的1124例患者中,1016例(90.39%)患者有导管数据。共插入91根(8.96%)锁骨下、387根(38.09%)颈内和538根(52.95%)股静脉透析导管。与其他两组相比,股静脉组患者更年轻(58.39±16.27),出血倾向更大[血小板计数更低(96.00±109.35),国际标准化比值更高(2.01±2.19)],入院时序贯器官衰竭评估基线评分更高(14.59±3.61)。本研究中透析导管相关并发症发生率较低,所有导管位置的并发症发生率无显著差异。在倾向评分和中心校正后,锁骨下组的死亡率和透析依赖率最低,而股静脉组的透析剂量(Kt/V)仍然最低。
患者特征会影响透析导管位置的选择,倾向于在更年轻、病情更重且凝血功能障碍更严重的患者中置入股静脉导管。尽管股静脉导管在间歇性血液透析期间可能与较低的透析剂量相关,但三种导管位置的并发症发生率在统计学上无显著差异。