He Zhenqiu, Xu Nan, Qi Sihua
Department of Anaesthesiology, The Fourth Affiliated Hospital of Harbin Medical University, Harbin, China.
Medicine (Baltimore). 2017 Apr;96(17):e6719. doi: 10.1097/MD.0000000000006719.
Cognitive function impairment is one of the most common complications in elderly patients after surgery, and an ideal nonpharmacological therapy has not yet been identified. Thus, we hypothesized that remote ischemic preconditioning could improve cognitive functions in elderly patients after surgery and investigated the mechanism underlying this effect.
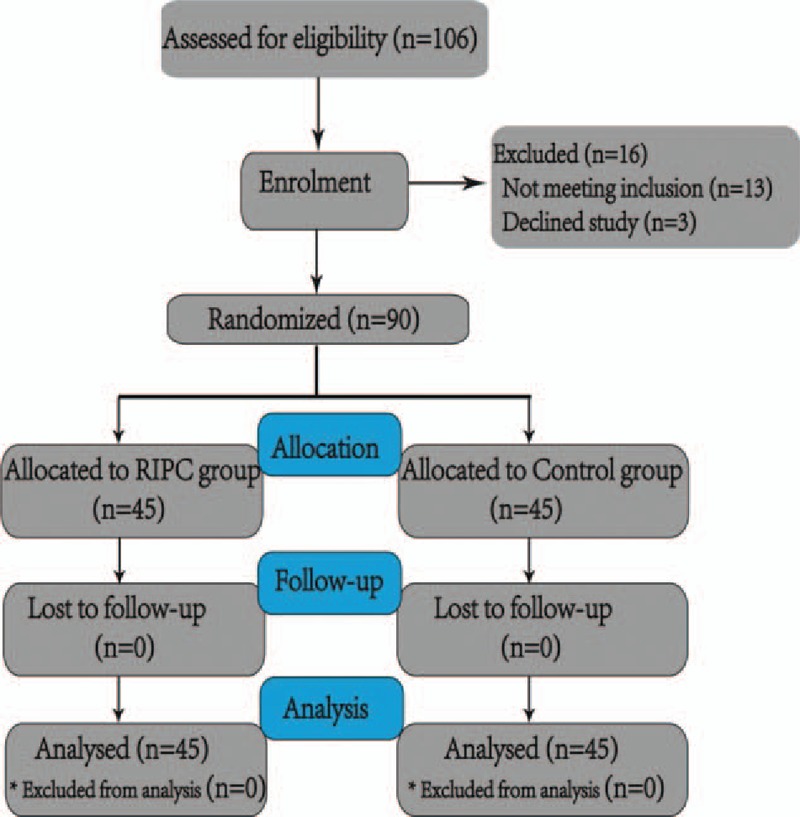
Ninety patients classified as American Society of Anaesthesiologists (ASA) physical status of 2 or 3 and aged 65 to 75 years who were scheduled for elective colon surgery under general anesthesia were randomly allocated to either a remote ischemic preconditioning group (Group R, n = 45) or a control group (Group C, n = 45). Remote ischemic preconditioning was performed by applying a static pressure of 200 mm Hg with a blood pressure cuff wrapped around the right upper limb for 3 ischemia cycles of 5 minutes each.
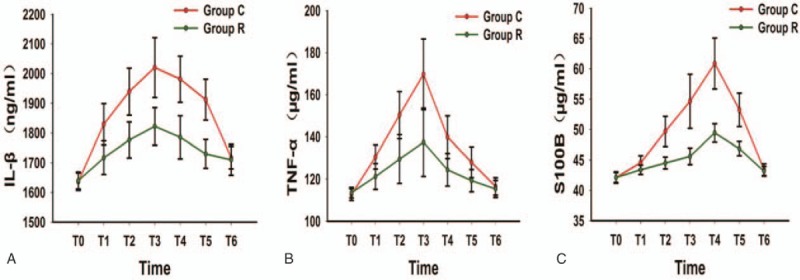
The Montreal Cognitive Assessment (MoCA) scores between the 2 groups were not significantly different on the day before surgery or the seventh day after surgery, but the scores on the first day after surgery (26.87 ± 0.84 vs 25.96 ± 0.85, P < .001) and third day after surgery (27.49 ± 0.66 vs 27.02 ± 0.92, P = .009) were significantly higher for Group R than those for Group C. Moreover, remote ischemic preconditioning markedly decreased the serum concentrations of the interleukin-1β (IL-1β), tumor necrosis factor-α (TNF-α), and S100B proteins compared with the control group (P < .001).
Remote ischemic preconditioning improves postoperative cognitive function in elderly patients following colon surgery. The cognitive protective effects of remote ischemic preconditioning are partially related to the inhibition of inflammation.
认知功能障碍是老年患者术后最常见的并发症之一,目前尚未确定理想的非药物治疗方法。因此,我们假设远程缺血预处理可以改善老年患者术后的认知功能,并研究其作用机制。
将90例年龄在65至75岁、美国麻醉医师协会(ASA)身体状况为2或3级、计划在全身麻醉下进行择期结肠手术的患者随机分为远程缺血预处理组(R组,n = 45)和对照组(C组,n = 45)。通过将血压袖带缠绕在上肢右侧并施加200 mmHg的静态压力5分钟,进行3个缺血周期,以实施远程缺血预处理。
两组患者在手术前一天或术后第七天的蒙特利尔认知评估(MoCA)评分无显著差异,但R组患者术后第一天(26.87 ± 0.84 vs 25.96 ± 0.85,P <.001)和术后第三天(27.49 ± 0.66 vs 27.02 ± 0.92,P =.009)的评分显著高于C组。此外,与对照组相比,远程缺血预处理显著降低了白细胞介素-1β(IL-1β)、肿瘤坏死因子-α(TNF-α)和S100B蛋白的血清浓度(P <.001)。
远程缺血预处理可改善老年结肠手术后患者的术后认知功能。远程缺血预处理的认知保护作用部分与炎症抑制有关。